- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Clinical Examination - Gait, Arms, Legs, Spine

急性坏疽阑尾炎的手术治疗
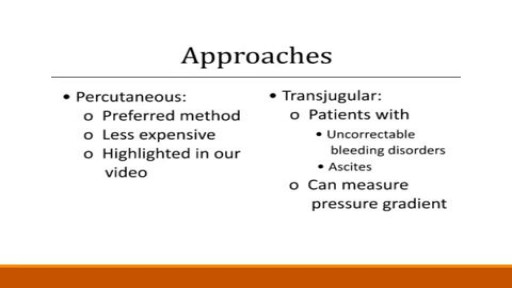
Renal artery stenosis is a narrowing of arteries that carry blood to one or both of the kidneys. Most often seen in older people with atherosclerosis (hardening of the arteries), renal artery stenosis can worsen over time and often leads to hypertension (high blood pressure) and kidney damage.

This video shows a patient with a large squamous cell carcinoma that has eroded through his external ear. The lesion has also infiltrated the parotid gland. We show the resection of this lesion with associated reconstruction.

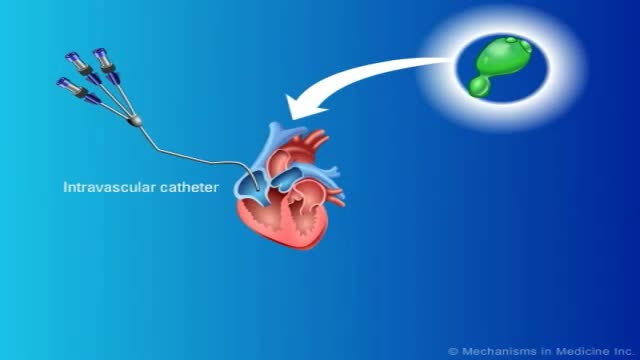
The fetal circulation is the circulatory system of a human fetus, often encompassing the entire fetoplacental circulation that also includes the umbilical cord and the blood vessels within the placenta that carry fetal blood.
The fetal circulation works differently from that of born humans, mainly because the lungs are not in use: the fetus obtains oxygen and nutrients from the mother through the placenta and the umbilical cord.

Most people develop several moles (nevi) throughout adulthood. Moles can be found anywhere on the body, usually in sun-exposed areas, and are usually brown, smooth, and slightly raised. In most cases, a nevus is benign and doesn't require treatment. Rarely, they turn into melanoma or other skin cancers. A nevus that changes shape, grows bigger, or darkens should be evaluated for removal.

Hydatid cysts in retroperitoneal region in transit to the thorax

Watch that video to know if Does Circumcision Affect Male Orgasm?

Fungal infections in bone marrow transplant patients. PURPOSE OF REVIEW: Invasive fungal infections have become the leading infectious cause of death in recipients of hematopoietic cell transplantation. Several factors have led to a renaissance in the study of invasive fungal infections.

Shane Shapiro, M.D., orthopedic physician at Mayo Clinic in Florida, performs a bone marrow aspiration and concentration for BMAC/stem cell injection into arthritic knees. This procedure is part of a Mayo Clinic IRB approved, FDA monitored clinical research trial which can be searched on at http://ClinicalTrials.gov.
Mayo Clinic and the Mayo Center for Regenerative Biotherapeutics is studying biologically based non-surgical treatments for osteoarthritis. One such treatment is the harvesting of the patient's own stem cells from their bone marrow.
"In our procedure we draw cellular rich bone marrow from both sides of the pelvis. We then filter the resulting product and concentrate the stem cells and their corresponding growth factors. Using an ultrasound to image the knee joint, we are then able to precisely inject the cells into the arthritic knee. We are currently demonstrating that this procedure is safe and can relieve pain. We also hope to be able to slow the progression of the degenerative joint disease and perhaps one day regrow cartilage in the arthritic joint."
------
Hear Dr. Shapiro discus this procedure in detail here: http://youtu.be/8Djpsc66hKI
Learn more about the Mayo Clinic Center for Regenerative Biotherapeutics here: http://goo.gl/rnRdtU
------
Mayo Clinic...
On Facebook: http://Facebook.com/MayoClinic
On Twitter: http://twitter.com/MayoClinic
On Google+: http://google.com/+MayoClinic
On Instagram: http://instagram.com/MayoClinic
On Pinterest: http://Pinterest.com/MayoClinic
On YouTube: http://YouTube.com/MayoClinic
On the blogs: http://connect.MayoClinic.org

St. Luke's originally broadcast this live in a webcast and later re-purposed it for air on KCRG-TV9 as an educational video. It is hosted by Ashley Hinson, KCRG-TV9 anchor and Dr. Sandeep Munjal. Dr. Jeff Nassif performs the knee replacement surgery on an eastern Iowa woman. St. Luke's has a rapid recovery joint replacement program, which gets people back to life quickly after surgery.

Dr. James Wall performs a bilateral inguinial hernia repair surgical procedure.
Featured:
James Wall, MD
Assistant Professor of Surgery, Pediatric Surgery
Assistant Professor of Bioengineering (By Courtesy)
Lucile Salter Packard Children's Hospital
Micaela Esquivel, MD
Chief Resident of General Surgery

TV interview with Dr. Mostafa Yakoot, MD discussing his recently published study for efficacy of lettuce seed oil in patients with insomnia
A sleep disorder, or somnipathy, is a medical disorder of the sleep patterns of a person or animal. Some sleep disorders are serious enough to interfere with normal physical, mental, social and emotional functioning. Polysomnography and actigraphy are tests commonly ordered for some sleep disorders.
People with lactose intolerance are unable to fully digest the sugar (lactose) in milk. As a result, they have diarrhea, gas and bloating after eating or drinking dairy products. The condition, which is also called lactose malabsorption, is usually harmless, but its symptoms can be uncomfortable. A deficiency of lactase — an enzyme produced in your small intestine — is usually responsible for lactose intolerance. Many people have low levels of lactase but are able to digest milk products without problems. If you're actually lactose intolerant, though, your lactase deficiency leads to symptoms after you eat dairy foods.
Dementia is the name for a group of symptoms that commonly include problems with memory, thinking, problem solving, language and perception. In a person with dementia, these symptoms are bad enough to affect daily life.

External ring Invagination
Internal ring occlusion test
History Inspection Palpation
taxis
Zieman

