- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
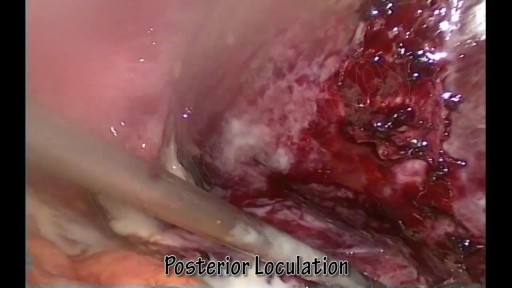
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

For more information on peritoneal dialysis: https://www.massgeneralbrigham.....org/en/about/newsro
Why does someone need dialysis? What is peritoneal dialysis? How does it work? John Kevin Tucker, M.D., Nephrologist at Brigham and Women's Hospital and Vice President for Education at Mass General Brigham, discusses peritoneal dialysis and its benefits for people who have lost their kidney function.
Subscribe Link: https://www.youtube.com/channe....l/UCYrLjATd88gPwIKnt
0:00 - Intro
0:24 - Why Do I Need Dialysis?
1:42 - Treatment
2:02 - Why Is It Called Peritoneal Dialysis
2:35 - 2 Forms of Peritoneal Dialysis
3:50 - Continuous Cycling Peritoneal Dialysis
4:38 - Myths
5:55 - Preparing For Peritoneal Dialysis
About Mass General Brigham:
Mass General Brigham combines the strength of two world-class academic medical centers, five nationally ranked specialty hospitals, 11 community hospitals, and dozens of health centers. Our doctors and researchers accelerate medical breakthroughs and drive innovations in patient care. They are leaders in medical education, serving as Harvard Medical School faculty and training the next generation of physicians. Mass General Brigham’s mission is to deliver the best, affordable health care to patients everywhere. Together, we transform the health of our communities and beyond.
#MassGeneralBrigham #Peritoneal #Dialysis
Visit Mass General Brigham: https://www.massgeneralbrigham.org/
Find us on social:
Twitter: https://twitter.com/MassGenBrigham
Instagram: https://www.instagram.com/massgeneralbrigham/
Facebook: https://www.facebook.com/MassGeneralBrigham/
LinkedIn: https://www.linkedin.com/compa....ny/mass-general-brig
Mass General Brigham:
https://www.youtube.com/massgeneralbrigham
Peritoneal Dialysis: At Home Treatment for Kidney Failure | Mass General Brigham
https://youtu.be/of1T6hMEN_Q

At URBN Dental, we offer the best dental services and highest quality care for your gum tissue health. Proper flossing techniques prevent your gum tissue from swelling, which often occurs from food and debris catching between your teeth. A routine dental cleaning every 6 months is recommended to maintain gum tissue health. Skipping bi annual checkups and improper flossing techniques often lead to periodontal disease which usually require a dental deep cleaning to undo tissue damage.

Mr Bean visits the hospital for a very peculiar reason!
A liver abscess is a pus-filled mass inside the liver. Common causes are abdominal infections such as appendicitis or diverticulitis due to haematogenous spread through the portal vein. A pyogenic liver abscess (PLA) is a pocket of pus that forms in the liver in response to an infection or trauma. Pus is a fluid composed of white blood cells, dead cells, and bacteria that forms when your body fights off infection.Dec 11, 2015
New Hemorrhoids Treatment Method
Full examination of the female from head to toe by Loyola Medical School, Chicago part 1

• Define and use related medical terminology.
• Describe and demonstrate techniques for imaging the thyroid gland.
• Discuss functional abnormalities of the thyroid gland.
• Correlate laboratory data relevant to the thyroid and parathyroid glands.
• Describe, and recognize on images, pathologies of the thyroid gland.
• Identify the anatomy of the parathyroid glands on diagrams and sonograms.
• Describe and demonstrate techniques for imaging the parathyroid glands.
• Describe, and recognize on images, pathologies of the parathyroid glands.
• List and describe other neck masses.
• Follow relevant protocols when scanning.
• Differentiate the sonographic appearances of the female reproductive organs in relation to the menstrual cycle, the use of contraceptives and hormone replacement, and following chemotherapy.
• Explain the Patient Privacy Rule (HIPAA) and Patient Safety Act (see reference).
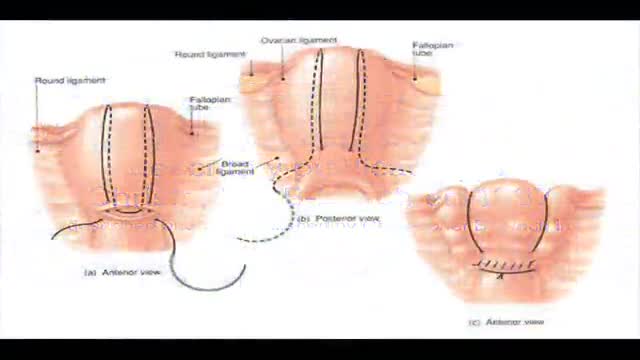
B-Lynch suture for uterine atony technique described

Rhinoplasty enhances facial harmony and the proportions of your nose. It can also correct impaired breathing caused by structural defects in the nose. Rhinoplasty surgery can change: Nose size in relation to facial balance Nose width at the bridge or in the size and position of the nostrils Nose profile with visible humps or depressions on the bridge Nasal tip that is enlarged or bulbous, drooping, upturned or hooked Nostrils that are large, wide, or upturned Nasal asymmetry If you desire a more symmetrical nose, keep in mind that everyone’s face is asymmetric to some degree. Results may not be completely symmetric, although the goal is to create facial balance and correct proportion.
Using state of the art 3D animation techniques, this video shows the anatomy of the heart. Includes close ups of the superior vena cava, rights and left atrium, the valves, the ventricles and the pulmonary artery.
Please note: this video contains no audio description or captions.
Your heart is an extraordinary machine - enjoy the visual showing you how it works :)
Copyright - Arcreative
Curious about medical device 3D animation? ➜ http://www.arcreative-media.com
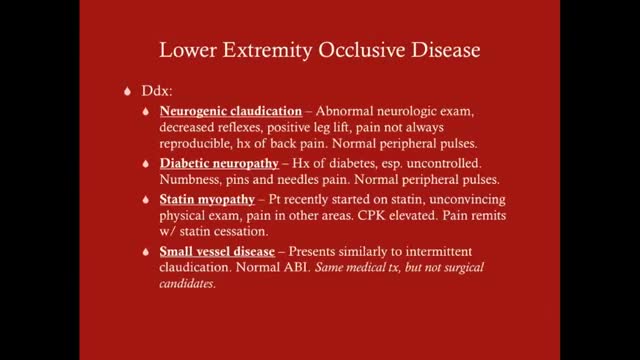
Claudication, which is defined as reproducible ischemic muscle pain, is one of the most common manifestations of peripheral arterial occlusive disease (PAOD) caused by atherosclerosis. Claudication occurs during physical activity and is relieved after a short rest. Pain develops because of inadequate blood flow. Examination of a patient with claudication should include a complete lower-extremity evaluation and pulse examination, including measuring segmental pressures. Attempt to palpate pulses from the abdominal aorta to the foot, with auscultation for bruits in the abdominal and pelvic regions. When palpable pulses are not present, a handheld Doppler device may be used to assess circulation.
If you have a lung disease, a type of surgery called a lobectomy is one treatment option your doctor may suggest. Your lungs are made up of five sections called lobes. You have three in your right lung and two in your left. A lobectomy removes one of these lobes. After the surgery, your healthy tissue makes up for the missing section, so your lungs should work as well or better than they did before.
High blood pressure is a common condition in which the long-term force of the blood against your artery walls is high enough that it may eventually cause health problems, such as heart disease. Blood pressure is determined both by the amount of blood your heart pumps and the amount of resistance to blood flow in your arteries. The more blood your heart pumps and the narrower your arteries, the higher your blood pressure. You can have high blood pressure (hypertension) for years without any symptoms. Even without symptoms, damage to blood vessels and your heart continues and can be detected. Uncontrolled high blood pressure increases your risk of serious health problems, including heart attack and stroke. High blood pressure generally develops over many years, and it affects nearly everyone eventually. Fortunately, high blood pressure can be easily detected. And once you know you have high blood pressure, you can work with your doctor to control it.

Lumpectomy means that a focal area of cancer is going to be removed. A lot of patients with a lumpectomy don’t need any specific breast reconstruction, explains Dr. Miguel Angel Medina, Director of Microsurgery with Miami Cancer Institute.
Al the end of surgical treatment, all those patients go on to need radiation therapy. For patients who have large breasts, physicians have to take a larger lumpectomy than normal.

Lattrell Wells was a perfect candidate for the MACI procedure. Dr. Michael O'Malley is a sports medicine surgeon at Carilion Clinic, "It’s a two stage procedure. So what we do is we actually harvest a small portion of the patient's cartilage and bone cells and we send it to a lab where the lab then that grows additional cartilage cells. It comes back to us in a little sheet and six weeks after that initial surgery, we re-implant the cartilage in a second surgery where we implant that sheet depending on the size of lesion right where his defect. This the only option where there’s virtually no risk of any kind of graft rejection or anything of that nature.

A surgical video showing Femoro-Popliteal Bypass with a Saphenous Vein Graft

http://www.landging.com/accident-animation-sports-injury-soccer.html
This accident animation demonstrates sports injury in soccer game.

A flail chest occurs when a segment of the thoracic cage is separated from the rest of the chest wall. This is usually defined as at least two fractures per rib (producing a free segment), in at least two ribs. A segment of the chest wall that is flail is unable to contribute to lung expansion. Large flail segments will involve a much greater proportion of the chest wall and may extend bilaterally or involve the sternum. In these cases the disruption of normal pulmonary mechanics may be large enough to require mechanical ventilation.
A colonoscope is the special tool used to perform a colonoscopy. It is a thin, flexible, tubular ‘telescope’ with a light and video camera that your doctor carefully guides through your colon in order to see and determine the health of your colon. Watch this animation to learn about the features of the colonoscope, how the colonoscopy procedure is performed and how polyps are removed, and the follow-up care you and your doctor should talk about after your procedure.

It flattens the natural curve of the spine, which can lead to lower back pain. Sleeping all night with the head turned to one side also strains the neck. If this is the preferred position, try using pillows to gradually train the body to sleep on one side
