- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
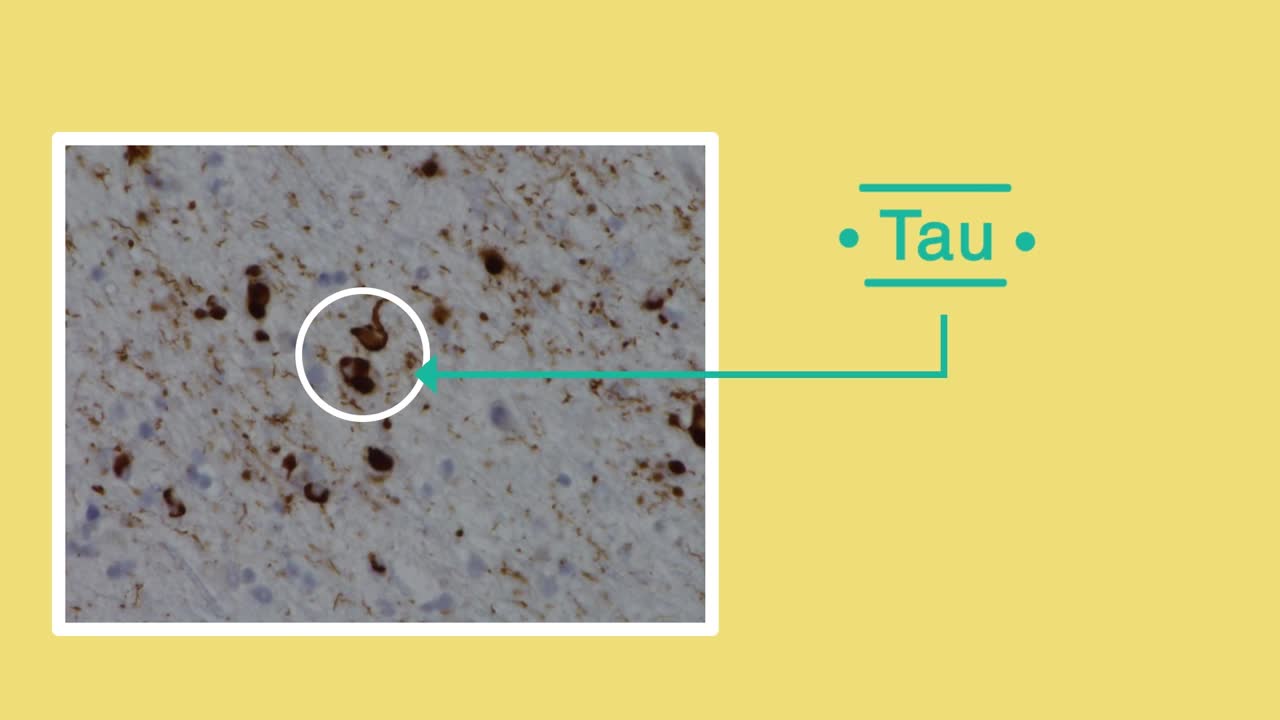
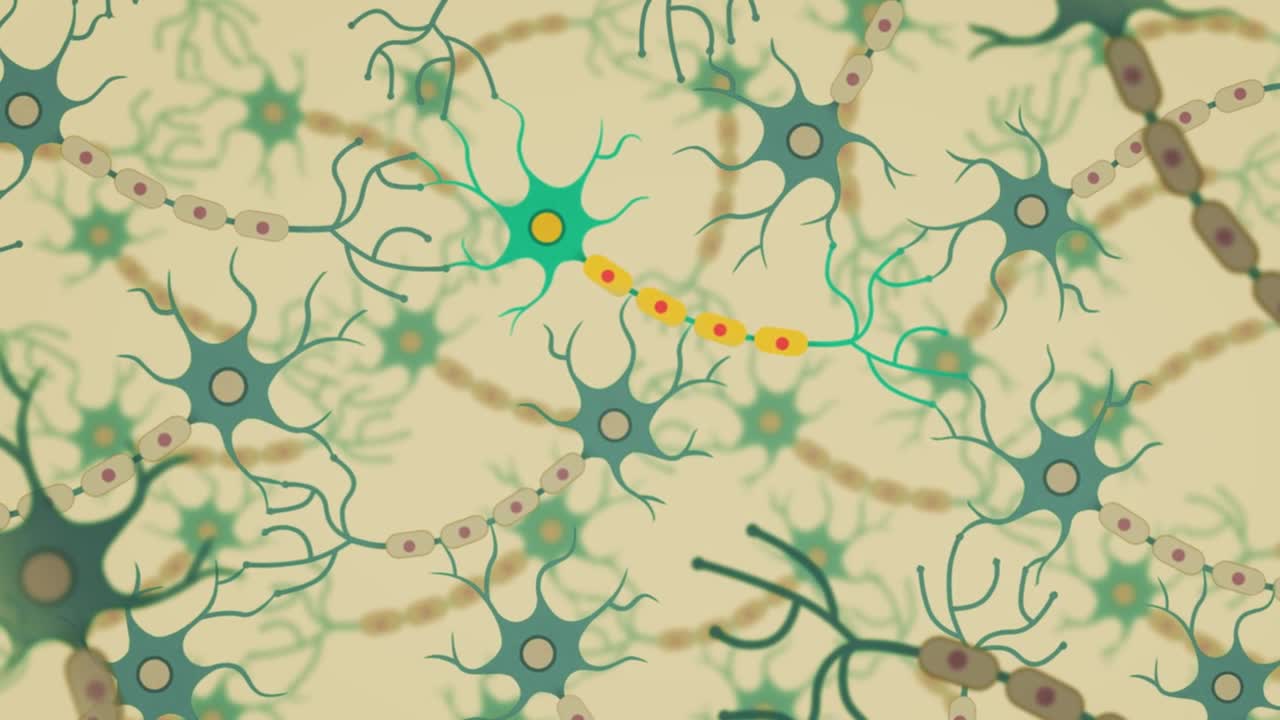
Frontotemporal dementia is the name for a range of conditions in which cells in the frontal and temporal lobes of the brain are damaged. These lobes control behaviour, emotional responses and language. This means that people will experience changes in personality and behaviour, or may struggle with language – for example, in finding the right word. Frontotemporal dementia is a less common form of dementia which is more likely to affect younger people – those under 65.
Dementia is the name for a group of symptoms that commonly include problems with memory, thinking, problem solving, language and perception. In a person with dementia, these symptoms are bad enough to affect daily life.

Renal artery stenosis is a narrowing of arteries that carry blood to one or both of the kidneys. Most often seen in older people with atherosclerosis (hardening of the arteries), renal artery stenosis can worsen over time and often leads to hypertension (high blood pressure) and kidney damage.

Watch that video to know if Does Circumcision Affect Male Orgasm?

Hydatid cysts in retroperitoneal region in transit to the thorax

Alcoholic hepatitis is inflammation of the liver caused by drinking alcohol. Alcoholic hepatitis is most likely to occur in people who drink heavily over many years. However, the relationship between drinking and alcoholic hepatitis is complex. Not all heavy drinkers develop alcoholic hepatitis, and the disease can occur in people who drink only moderately. If you're diagnosed with alcoholic hepatitis, you must stop drinking alcohol. People who continue to drink alcohol face a high risk of serious liver damage and death.

Shane Shapiro, M.D., orthopedic physician at Mayo Clinic in Florida, performs a bone marrow aspiration and concentration for BMAC/stem cell injection into arthritic knees. This procedure is part of a Mayo Clinic IRB approved, FDA monitored clinical research trial which can be searched on at http://ClinicalTrials.gov.
Mayo Clinic and the Mayo Center for Regenerative Biotherapeutics is studying biologically based non-surgical treatments for osteoarthritis. One such treatment is the harvesting of the patient's own stem cells from their bone marrow.
"In our procedure we draw cellular rich bone marrow from both sides of the pelvis. We then filter the resulting product and concentrate the stem cells and their corresponding growth factors. Using an ultrasound to image the knee joint, we are then able to precisely inject the cells into the arthritic knee. We are currently demonstrating that this procedure is safe and can relieve pain. We also hope to be able to slow the progression of the degenerative joint disease and perhaps one day regrow cartilage in the arthritic joint."
------
Hear Dr. Shapiro discus this procedure in detail here: http://youtu.be/8Djpsc66hKI
Learn more about the Mayo Clinic Center for Regenerative Biotherapeutics here: http://goo.gl/rnRdtU
------
Mayo Clinic...
On Facebook: http://Facebook.com/MayoClinic
On Twitter: http://twitter.com/MayoClinic
On Google+: http://google.com/+MayoClinic
On Instagram: http://instagram.com/MayoClinic
On Pinterest: http://Pinterest.com/MayoClinic
On YouTube: http://YouTube.com/MayoClinic
On the blogs: http://connect.MayoClinic.org
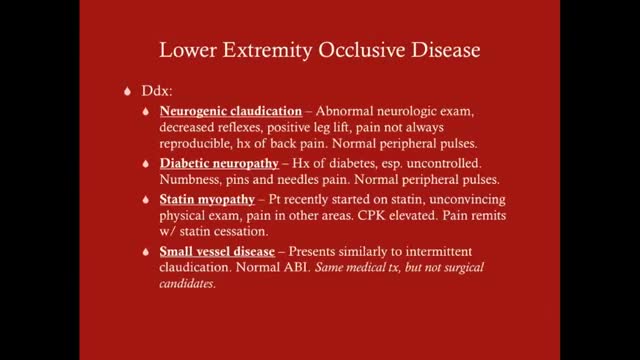
Claudication, which is defined as reproducible ischemic muscle pain, is one of the most common manifestations of peripheral arterial occlusive disease (PAOD) caused by atherosclerosis. Claudication occurs during physical activity and is relieved after a short rest. Pain develops because of inadequate blood flow. Examination of a patient with claudication should include a complete lower-extremity evaluation and pulse examination, including measuring segmental pressures. Attempt to palpate pulses from the abdominal aorta to the foot, with auscultation for bruits in the abdominal and pelvic regions. When palpable pulses are not present, a handheld Doppler device may be used to assess circulation.
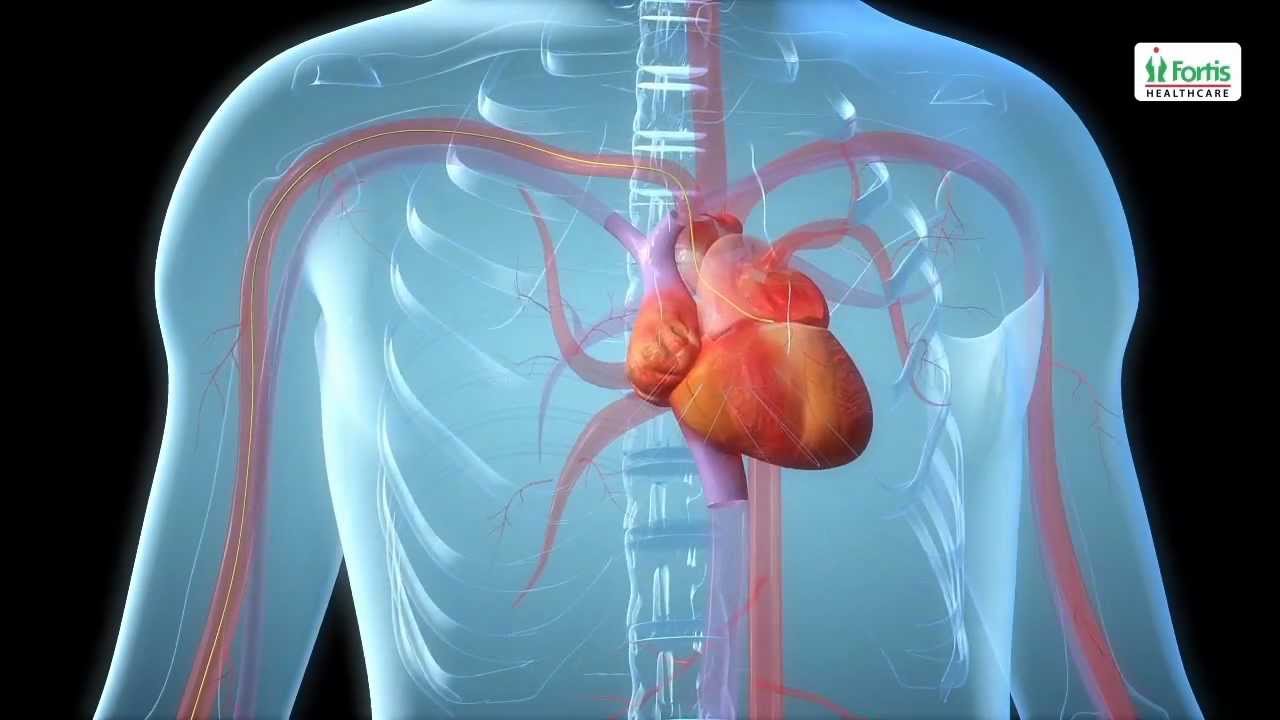
Angioplasty Procedure Animation Video
Emergency angioplasty is an operation that is performed directly after a heart attack, on admission to the hospital. It involves the insertion of a catheter into the blocked blood vessel that caused the heart attack. This opens it up and allows blood to flow again, thus minimizing damage to the heart.
If one or more arteries become clogged, it may result in a heart attack. This normally presents with chest pain, sweating and a feeling of anxiety, among other symptoms. Urgent medical assistance should be sought. A heart attack is a medical emergency requiring intervention as soon as possible.
Know more: http://www.emergencyangioplasty.com/
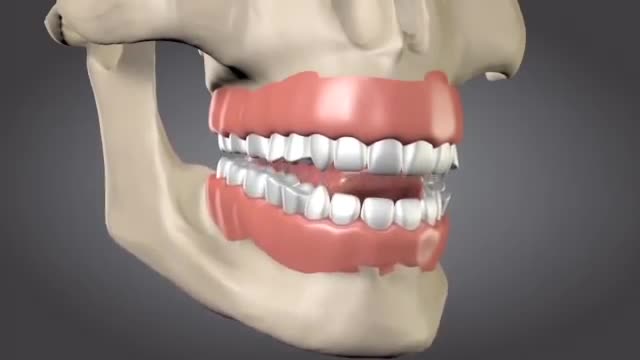
Tooth loss can make you look older. When you lose a tooth and don’t replace it with a dental implant, you risk the chance of jawbone loss. Normally, your tooth root stimulates the continued growth and health of your jawbone. Dental implants mirror your natural tooth root and keep your jawbone healthy.
People with lactose intolerance are unable to fully digest the sugar (lactose) in milk. As a result, they have diarrhea, gas and bloating after eating or drinking dairy products. The condition, which is also called lactose malabsorption, is usually harmless, but its symptoms can be uncomfortable. A deficiency of lactase — an enzyme produced in your small intestine — is usually responsible for lactose intolerance. Many people have low levels of lactase but are able to digest milk products without problems. If you're actually lactose intolerant, though, your lactase deficiency leads to symptoms after you eat dairy foods.
Ejaculating into a partner’s mouth is a common practice during oral sex/fellatio. In a safe situation (where there is no danger of catching an STD), the semen-receiving partner may choose to spit the semen out, or to swallow it. Before you engage in fellatio, I’d recommend that you and your partner both get tested for sexually transmitted infections (STIs). If not, please use barriers for oral sex and abstaining from making contact with ejaculate. Semen is mostly water, but also contains amino acids and protein, sugars such as fructose and glucose, minerals such as zinc and calcium, vitamin C, and a few other nutrients. Sperm cells themselves make up less than one percent of semen. Semen is edible, and if swallowed, will travel down the esophagus and into the stomach, where it will be digested in the same way that food is. You can never get pregnant by swallowing semen. Some people accept the taste of semen, but others complain that swallowing semen can give them an upset stomach. In rare cases, you may have an allergy to the proteins found in semen. What does It Taste Like? The taste of semen varies. Bitter, sweet, metallic. So, one may expect to find the taste of semen anywhere from enjoyable to tasteless to disgusting. But there is a way of controlling the taste of semen, which is through diet. Keep track of the diet, and communicate with the partner about when it tastes better or worse.

An inguinal hernia occurs when tissue, such as part of the intestine, protrudes through a weak spot in the abdominal muscles. The resulting bulge can be painful, especially when you cough, bend over or lift a heavy object. However, many hernias do not cause pain.
An inguinal hernia isn't necessarily dangerous. It doesn't improve on its own, however, and can lead to life-threatening complications. Your doctor is likely to recommend surgery to fix an inguinal hernia that's painful or enlarging. Inguinal hernia repair is a common surgical procedure.

Choking Child Video Demonstration

急性坏疽阑尾炎的手术治疗

Watch that video to know What is Vaginal Discharge and How To Get Rid of It

Gallbladder "Lumigram" - shows the common bile duct(being probed) and the cystic duct (the duct YOU WANT TO CUT)

Clinical Examination - Gait, Arms, Legs, Spine
