- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

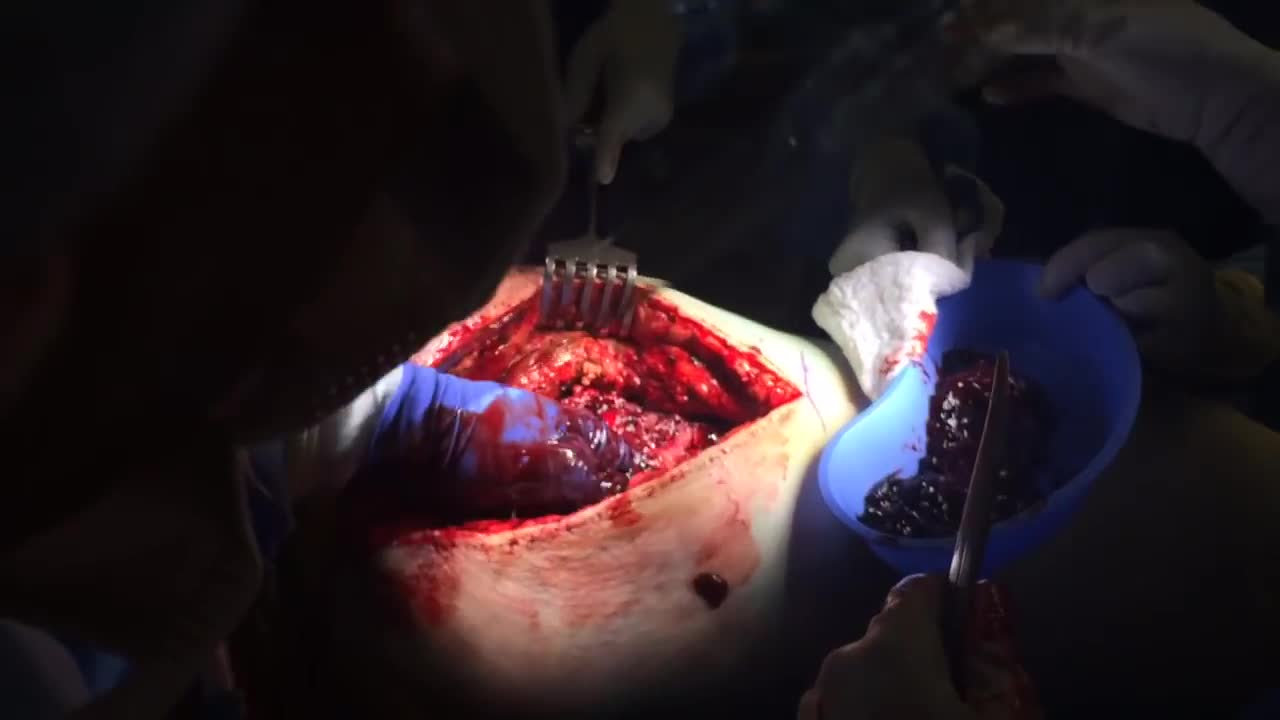
急性坏疽阑尾炎的手术治疗
A hematoma is a common complication of surgical procedures. A large, expanding hematoma can result in necrosis of the overlying skin (1,2) or adjacent subcutaneous fat, increased incidence of infection, scarring, skin hyperpigmentation, tissue edema and a prolonged convalescence.

Clinical Examination - Gait, Arms, Legs, Spine

St. Luke's originally broadcast this live in a webcast and later re-purposed it for air on KCRG-TV9 as an educational video. It is hosted by Ashley Hinson, KCRG-TV9 anchor and Dr. Sandeep Munjal. Dr. Jeff Nassif performs the knee replacement surgery on an eastern Iowa woman. St. Luke's has a rapid recovery joint replacement program, which gets people back to life quickly after surgery.

For more videos, please visit:
http://surgicalfilmatlas.mssm.edu/

Most people develop several moles (nevi) throughout adulthood. Moles can be found anywhere on the body, usually in sun-exposed areas, and are usually brown, smooth, and slightly raised. In most cases, a nevus is benign and doesn't require treatment. Rarely, they turn into melanoma or other skin cancers. A nevus that changes shape, grows bigger, or darkens should be evaluated for removal.
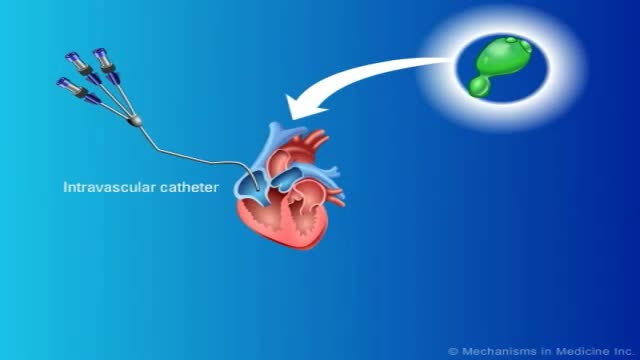
Renal artery stenosis is a narrowing of arteries that carry blood to one or both of the kidneys. Most often seen in older people with atherosclerosis (hardening of the arteries), renal artery stenosis can worsen over time and often leads to hypertension (high blood pressure) and kidney damage.

Watch that video to know if Does Circumcision Affect Male Orgasm?
Fungal infections in bone marrow transplant patients. PURPOSE OF REVIEW: Invasive fungal infections have become the leading infectious cause of death in recipients of hematopoietic cell transplantation. Several factors have led to a renaissance in the study of invasive fungal infections.
When the hematocrit rises to 60 or 70%, which it often does in polycythemia, the blood viscosity can become as great as 10 times that of water, and its flow through blood vessels is greatly retarded because of increased resistance to flow. This will lead to decreased oxygen delivery.

Choking Child Video Demonstration
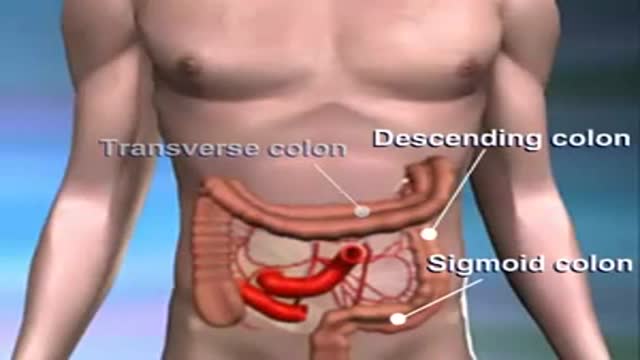
Colon cancer usually begins as a non-cancerous growth. If caught early enough, it can be safely removed with little to no complications.

At Nationwide Children’s, our Department of General Pediatric Surgery provides comprehensive surgical care for infants, children and adolescents with congenital and acquired conditions, including major congenital anomalies, traumatic and thermal injuries, and tumors. As the second largest pediatric treatment center in the United States our surgeons perform more than 4,000 operative procedures every year. We are dedicated to clinical excellence, generation of new knowledge through research and the training of the next generation of leaders in children’s surgery. Under the umbrella of a unified program, 11 surgical departments share a common mission, philosophy and approach to patient care.
Pediatric Surgery Program: https://bit.ly/3t4QZef
Pediatric Surgery Fellowship and Residency: https://bit.ly/3qWAWwd
Meet our Pediatric Surgery Team: https://bit.ly/3n39dJh
Fellowship Programs: https://bit.ly/3EX1JNX
Surgical Services: https://bit.ly/3eYDlB8

Gallbladder "Lumigram" - shows the common bile duct(being probed) and the cystic duct (the duct YOU WANT TO CUT)

TV interview with Dr. Mostafa Yakoot, MD discussing his recently published study for efficacy of lettuce seed oil in patients with insomnia

inspection, auscultation and palpation

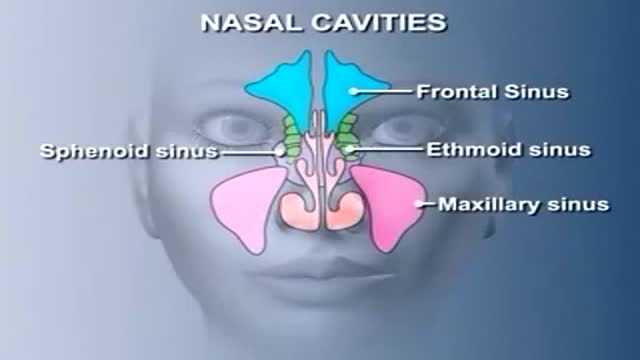
Nose Anatomy

Dr. Joanna Chikwe, explains how patients may feel after heart surgery.
Learn more about the Smidt Heart Institute at Cedars-Sinai at https://ceda.rs/3meIA2A
Learn more about Dr. Joanna Chikwe at https://ceda.rs/3ul6I6t
Connect with us:
https://twitter.com/CedarsSinai
https://www.facebook.com/CedarsSinai
https://www.instagram.com/CedarsSinai
Cedars-Sinai is a leader in providing high-quality healthcare encompassing primary care, specialized medicine and research. Since 1902, Cedars-Sinai has evolved to meet the needs of one of the most diverse regions in the nation, setting standards in quality and innovative patient care, research, teaching and community service. Today, Cedars- Sinai is known for its national leadership in transforming healthcare for the benefit of patients. Cedars-Sinai impacts the future of healthcare by developing new approaches to treatment and educating tomorrow’s health professionals. Additionally, Cedars-Sinai demonstrates a commitment to the community through programs that improve the health of its most vulnerable residents.

This video shows a patient with a large squamous cell carcinoma that has eroded through his external ear. The lesion has also infiltrated the parotid gland. We show the resection of this lesion with associated reconstruction.
