- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

If your levels are too low, you have hypothyroidism and may not be ovulating as you should. Taking the right dose of thyroxine, the hormone you lack, can restore your fertility. You may have discovered your underactive thyroid as a result of trying to get pregnant.

very funny medical video..DO NOT TRY AT CLINIC
Watch that video to know How to Get Pregnant Fast and Easy

Dr. Joanna Chikwe, explains how patients may feel after heart surgery.
Learn more about the Smidt Heart Institute at Cedars-Sinai at https://ceda.rs/3meIA2A
Learn more about Dr. Joanna Chikwe at https://ceda.rs/3ul6I6t
Connect with us:
https://twitter.com/CedarsSinai
https://www.facebook.com/CedarsSinai
https://www.instagram.com/CedarsSinai
Cedars-Sinai is a leader in providing high-quality healthcare encompassing primary care, specialized medicine and research. Since 1902, Cedars-Sinai has evolved to meet the needs of one of the most diverse regions in the nation, setting standards in quality and innovative patient care, research, teaching and community service. Today, Cedars- Sinai is known for its national leadership in transforming healthcare for the benefit of patients. Cedars-Sinai impacts the future of healthcare by developing new approaches to treatment and educating tomorrow’s health professionals. Additionally, Cedars-Sinai demonstrates a commitment to the community through programs that improve the health of its most vulnerable residents.

Learn about the structural unit of compact bone (the osteon) and it's four basic parts: central canal, lamellae, lacunae, and canaliculi

Most innovative dental implant system
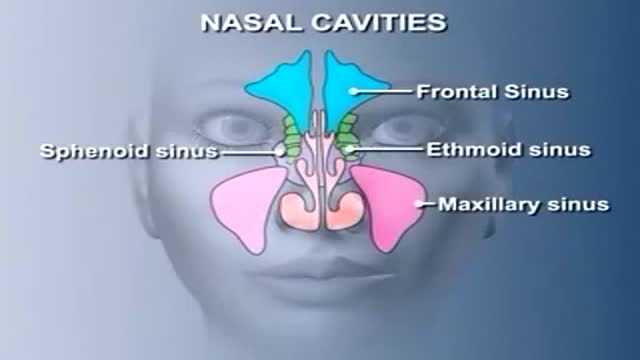
Nose Anatomy

Ellis demonstrates how to perform good hand hygiene with soap and water.
Our Critical Nursing Skills video tutorial series is taught by Ellis Parker MSN, RN-BC, CNE, CHS and intended to help RN and PN nursing students study for your nursing school exams, including the ATI, HESI and NCLEX.
#NCLEX #ClinicalSkills #HandHygiene #HESI #Kaplan #ATI #NursingSchool #NursingStudent #Nurse #RN #PN #Education #LVN #LPN #nurseeducator
00:00 What Is Good Hand Hygiene?
00:27 Prepping to wash hands
01:01 Proper hand washing technique
01:53 How to dry hands
02:14 Proper technique to turn off faucet
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.00:00 Good Hand Hygiene?

Watch that video to know How to Get Rid of Saggy Breasts Naturally

The "Get up and go" test is most commonly used to assess postural stability. In this test, the physician instructs the patient to stand up from a chair without assistance, walk a short distance, turn around, return, and sit down again. If the patient is unsteady or has difficulties during the test, further evaluation is necessary.

Big wart blister after freezing with liquid nitrogen.

Choking Child Video Demonstration

Gallbladder "Lumigram" - shows the common bile duct(being probed) and the cystic duct (the duct YOU WANT TO CUT)

inspection, auscultation and palpation

Breast augmentation usually is performed in subglandular, subfascial, or partial submuscular pockets, including the dual plane. A new pocket has been described and used by the author. Methods: From October 2005 to April 2008, 600 patients underwent bilateral breast augme...
ntation using the new technique. Soft cohesive gel micro-textured round implants (range 200- 500cc) were used. The initial pocket is made in the subglandular plane up to the lower level of the nipple areolar complex. The submuscular plane is reached by splitting the pectoralis major muscle at the level of middle and lower third of sternum. The muscle is split along the direction of its fibers up and laterally to the anterior axillary fold. No pectoralis major is released from costal margin. The implant lies in this plane simultaneously behind and in front of the pectoralis major. Procedure is performed as a day case under general anesthetic with no drains. Results: Postoperative analgesia requirements is reduced because of dissection in natural planes resulting in quick recovery. No muscle contraction associated deformities is seen. All patients had aesthetically natural cleavage, with the nipple at the most projected part of the breast with three-dimensional enhancement. Conclusion: An adequate muscle cover of the prosthesis is achieved by muscle splitting breast augmentation technique and the procedure is used in all breast augmentations procedures

Diastasis recti often occurs during pregnancy and can persist after pregnancy. It affects core strength and the appearance of the abdominal muscles.
Dr. Erick Sanchez repairs the abdominal muscles with every tummy tuck. This short video shows the muscle repair portion of the surgery with a bonus after photo at the end!
To request a consultation with Dr. Sanchez, visit sanchezplasticsurgery.com and click Request a Consultation. Fill out the form and someone will get in touch with you to answer all your questions.
Expected cost can be found at the bottom of each procedure page on our website.

Colonoscopy Showing Moving Parasites

This video shows a patient with a large squamous cell carcinoma that has eroded through his external ear. The lesion has also infiltrated the parotid gland. We show the resection of this lesion with associated reconstruction.
Open heart (coronary artery bypass, or CABG) surgery is performed in order to reroute, or "bypass," blood around blocked arteries, thereby improving the supply of oxygen-rich blood to the heart. Surgeons usually use an artery from the chest wall to construct the "detour" around the blocked part of the artery. Veins from the legs are also used.

TV interview with Dr. Mostafa Yakoot, MD discussing his recently published study for efficacy of lettuce seed oil in patients with insomnia
