- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

In this video, I am talking about the best histology resources available on the internet. All the links to the resources I talked are here -
1. Amit's lectures - https://www.youtube.com/channe....l/UCwdAyZnA6FEE0Iqsw
2. VIBS histology - https://www.youtube.com/c/VIBSHistology/featured
3. Dr. Eman Sadek Histology Queen - https://www.youtube.com/channe....l/UCHXGb5GphBKKN-xD3
4. BIOC 21 Histology lectures - https://www.youtube.com/playli....st?list=PLKnI3Jl97pW
5. https://medicalschoolpathology.com/
7. Udemy - https://clnk.in/qfEB
Buy this awsm book for Histology - https://amzn.to/3wSX1Oh

An animation of blood flow inside the hollow fiber of a hemofilter, or a dialyzer, and the flow of the dialysate in an opposite direction with increased extraction of waste and small molecules from the blood as the concentration of these molecules is reduced downstream and exposed to new dialysate.
To learn about Hemodialysis..
https://www.thevirtualnephrolo....gist.com/specialties
The Virtual Nephrologist is your gateway to optimal health.
To learn more about Hypertension, Kidney Disease and Dialysis:
https://thevirtualnephrologist.com/
About Dr. Rifai:
Dr. Ahmad Oussama Rifai is certified by the American Board of Internal Medicine (ABIM) in the specialty of Internal Medicine and the sub-specialty of Nephrology.
MEET DR. RIFAI
https://www.thevirtualnephrologist.com/rifai/
Follow The Virtual Nephrologist on SOCIAL MEDIA:
-Facebook: https://www.facebook.com/thevirtualnephrologist
-Instagram: https://www.instagram.com/thevirtualnephrologist/
-Twitter: https://twitter.com/VNephrologist
-TikTok: https://www.tiktok.com/@thevirtualnephrologist
Schedule a virtual consult:
https://www.thevirtualnephrolo....gist.com/schedule-a-
Best wishes for great health | The Virtual Nephrologist
Upper right quadrant: The right upper quadrant contains the liver and gallbladder, which are protected by the lower right part of the ribcage. The large intestine, or colon, also spends a little time in this section. Upper left quadrant: The left upper quadrant contains part of the stomach and the spleen.

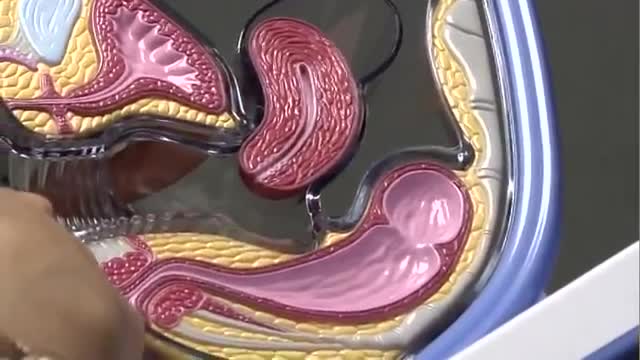
Dr. Daniel Del Vecchio, Harvard trained plastic surgeon, performs his breast lift technique, filling the upper portion of the breast for added volume
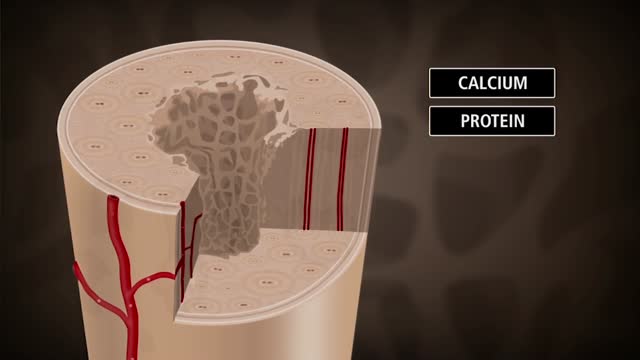
Bone is not a static part of the body — it's constantly being resorbed (broken down) and formed throughout your life. Your entire skeleton is replaced about every decade, according to the NIH. During your childhood and teenage years, bone formation occurs more quickly than bone resorption, resulting in growth. You reach your maximum bone density and strength around age 30, after which bone resorption slowly overtakes bone formation. Osteoporosis develops when there's an abnormal imbalance between bone resorption and formation — that is, resorption occurs too quickly, or formation too slowly.
plantar fasciitis and calcaneal spur can be treated by EPFR with calcanean drilling - endoscopic plantar fascia release علاج الشوكة العظمية للكعب بالمنظار د. أسامة الشاذلي مدرس جراحة العظام واستشاري جراحات و مناظير القدم والكاحل كلية الطب جامعة عين شمس

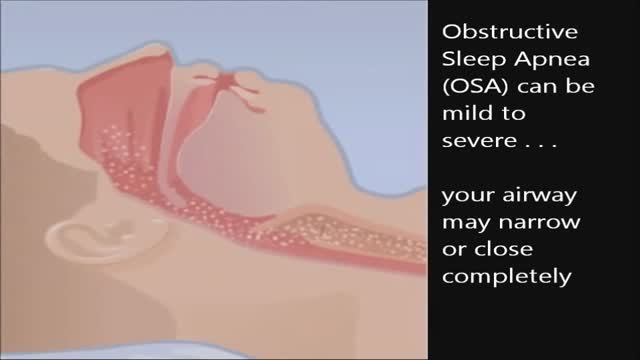
CPAP, or continuous positive airway pressure, is a treatment that uses mild air pressure to keep the airways open. CPAP typically is used by people who have breathing problems, such as sleep apnea. CPAP also may be used to treat preterm infants whose lungs have not fully developed.

جروب الداتا على #تليجرام 👇🏻
https://t.me/IslamKhalaf
أي استفسار 👇🏻
twitter
https://twitter.com/Islamkhalaf0
Insta
https://www.instagram.com/islamkhalaf1
FB
https://www.facebook.com/islamkhalaf.A

The Combitube is a twin lumen device designed for use in emergency situations and difficult airways. It can be inserted without the need for visualization into the oropharynx, and usually enters the esophagus. It has a low volume inflatable distal cuff and a much larger proximal cuff designed to occlude the oro- and nasopharynx.
If the tube has entered the trachea, ventilation is achieved through the distal lumen as with a standard ETT. More commonly the device enters the esophagus and ventilation is achieved through multiple proximal apertures situated above the distal cuff. In the latter case the proximal and distal cuffs have to be inflated to prevent air from escaping through the esophagus or back out of the oro- and nasopharynx.

Open Appendectomy Surgery Video

Acute hemothorax due to aortic rupture in aortic dissection with lung collapse and mediastinal shift.
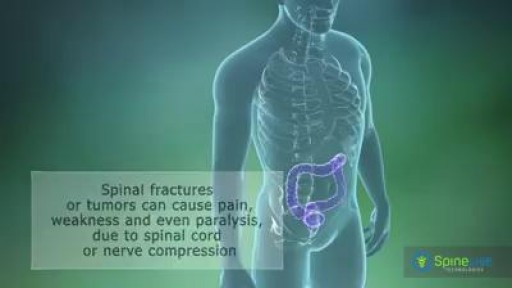
A spinal tumor is a growth that develops within your spinal canal or within the bones of your spine. It may be cancerous or noncancerous. Tumors that affect the bones of the spine (vertebrae) are known as vertebral tumors. Tumors that begin within the spinal cord itself are called spinal cord tumors. There are two main types of tumors that may affect the spinal cord: Intramedullary tumors begin in the cells within the spinal cord itself, such as astrocytomas or ependymomas. Extramedullary tumors develop within the supporting network of cells around the spinal cord. Although they don't begin within the spinal cord itself, these types of tumors may affect spinal cord function by causing spinal cord compression and other problems. Examples of extramedullary tumors that can affect the spinal cord include schwannomas, meningiomas and neurofibromas.

For Employees of Hospitals, Schools, Universities and Libraries: Download 8 FREE medical animations from Nucleus by signing up for a free trial: http://nmal.nucleusmedicalmedi....a.com/free-trial-mem
Biology students: Subscribe to the Nucleus Biology channel to see new animations on biology and other science topics, plus short quizzes to ace your next exam: https://bit.ly/3lH1CzV
This medical animation depicts Laser Eye Surgery, a procedure that permanently changes the shape of the cornea, the clear covering over the front of the eye.
#lasik #eye #cornea
ANCE00185
LASER PARA VASINHOS Veja mais em www.vascular.pro

The 12-lead ECG is a vital tool for EMT’s and paramedics in both the prehospital and hospital setting. It is extremely important to know the exact placement of each electrode on the patient. Incorrect placement can lead to a false diagnosis of infarction or negative changes on the ECG.

Inflammation of the uvula is known as uvulitis. Your uvula will appear red, puffy, and larger than normal. Other symptoms of uvulitis may include: itching burning a sore throat spots on your throat snoring difficulty swallowing trouble breathing If you have a swollen uvula along with a fever or abdominal pain, consult with your doctor right away. In rare cases, the uvula can swell enough to block your airway. Swelling of the throat is a life-threatening event. If this happens, seek immediate medical attention. What causes a swollen uvula? Causes Inflammation is your body’s response when it’s under attack. Triggers for inflammation include: environmental and lifestyle factors an infection trauma genetics Environmental and Lifestyle Factors The most common food allergies are peanuts tree nuts milk eggs wheat soy fish, including shellfish You could be having an allergic reaction to something you touched, swallowed, or breathed in. Some common allergens include: food irritants , such as dust, animal dander, or pollen medication exposure to chemicals or other toxic substances, including tobacco Infection You can get viral infections or bacterial infections. Examples of viral infections include: the common cold the flu mononucleosis chickenpox measles croup The most common bacterial infection is strep throat, which occurs due to Streptococcus pyogenes, which is a type of group A Streptococcus. If you have infected tonsils, or tonsillitis, severe inflammation can cause them to push against and irritate your uvula. Trauma Trauma to the uvula can happen if you need an intubation, such as during surgery. Your uvula can also be injured during a tonsillectomy. This is a procedure to remove your tonsils, which are located on both sides of your uvula. Your throat and uvula can also become irritated if you have acid reflux disease or if you vomit frequently. Genetics A condition called hereditary angioedema (HAE) can cause swelling of the uvula and throat, as well as swelling of the face, hands, and feet. Other symptoms include nausea, vomiting, and abdominal pain. It’s an uncommon genetic mutation that occurs in 1 in 10,000 to 1 in 50,000 people. It’s rare, but there are case reports of individuals who have an elongated uvula, which can also interfere with breathing. What are the risk factors for a swollen uvula? Risk Factors Anyone can get uvulitis, but adults get it less often than children do. You’re at increased risk if you: have allergies use tobacco products are exposed to chemicals and other irritants in the environment have a weakened immune system, making you more susceptible to infections How is a swollen uvula diagnosed? Diagnosis If you have fever or swelling of your throat, see your doctor. Be prepared to give a complete medical history. Tell your doctor: about all the over-the-counter and prescription medications you take if you’re a smoker or you chew tobacco if you’ve recently tried new foods if you’ve been exposed to chemicals or unusual substances about your other symptoms, such as abdominal pain, fever, or dehydration Your doctor may be able to make a diagnosis through a physical exam. It’s likely you’ll also need a throat swab to evaluate for strep or to obtain secretions for culture to determine if you have another bacterial or fungal infection. This test is known as the rapid strep test. You may also need a nasal swab to test for influenza. Blood testing can help identify or rule out some other infectious agents. If those tests are inconclusive, you may need to see an allergist. Blood and skin tests can help identify foods or other substances that cause a reaction. Learn more: Allergy testing » If necessary, imaging tests can provide a more detailed view of your throat and the surrounding area. What’s the treatment for a swollen uvula? Treatment When you have something like the common cold, swelling usually clears up on its own without treatment. Otherwise, treatment will depend on how severe your symptoms are, as well as what’s causing the inflammation. Infection Viral infections tend to clear up without treatment. The only upper respiratory infection for which an antiviral medication is available is influenza. Antibiotics can treat bacterial infections. Even after symptoms clear up, take all the medication as prescribed. If your condition may be contagious, stay home until your doctor tells you that you’re no longer at risk of spreading it to others. Allergy If you test positive for an allergy, try to avoid the allergen in the future. Doctors usually treat allergies with antihistamines or steroids. Anaphylaxis is a severe allergic reaction. Doctors use epinephrine to treat this reaction. Hereditary angioedema Your doctor may treat HAE with any of the following: anabolic steroids, or androgens antifibrinolytics C1 inhibitors, such as C1 esterase inhibitor (Berinert) or C1 esterase inhibitor (recombinant) (Ruconest) a plasma kallikrein inhibitor, such as ecallantide (Kalbitor) bradykinin receptor antagonist, such as icatibant injection (Firazyr) Tell your doctor if you have new or worsening symptoms, and follow up as necessary. Tips for relief home treatment If you have a swollen uvula or sore throat, it’s your body’s way of telling you that something is wrong. A few home remedies can help keep you strong and soothe your irritated throat. Make sure you’re getting enough fluids. If your throat hurts when you drink, try drinking small amounts throughout the day. Your urine should be light in color. If it’s dark yellow or brown, you’re not drinking enough and may be dehydrated. Additional tips include the following: Cool your throat by sucking on ice chips. Frozen juice bars or ice cream may also do the trick. Gargle with warm salt water to ease your dry, scratchy throat. Aim for a full night’s sleep, and nap during the day if you can. What’s the outlook? Outlook A swollen uvula isn’t a common occurrence. Most of the time it clears up without treatment. If you have an infection, prompt treatment should take care of the problem within a week or two. If you have allergies that lead to swelling of the uvula or throat, do your best to avoid that allergen. You should also be prepared to deal with an attack if you come into contact with the substance again. If you’ve ever had anaphylaxis, ask your doctor if you should carry injectable epinephrine (EpiPen) in case of emergency. People with HAE must learn to recognize triggers and early warning signs of an attack. Talk to your doctor about how to manage HAE. Article Resources Was this article helpful?Yes No Share Tweet Email Print Read This Next 9-Month-Old Baby: Developmental Milestones and Guidelines 9-Month-Old Baby: Developmental Milestones and Guidelines Read More » All of the ‘Firsts’ That Come with Breast-Feeding All of the ‘Firsts’ That Come with Breast-Feeding Read More » 5 Types of Health Professionals You Should Know About 5 Types of Health Professionals You Should Know About Read More » What’s the Difference Between a Fracture and a Break? What’s the Difference Between a Fracture and a Break? Read More » Is Corn a Vegetable? Is Corn a Vegetable? Read More » Advertisement Advertisement Advertisement
Postmenopausal bleeding (PMB) is defined for practical purposes as vaginal bleeding occurring after twelve months of amenorrhoea, in a woman of the age where the menopause can be expected.[1] Hence it does not apply to a young woman, who has had amenorrhoea from anorexia nervosa, or a pregnancy followed by lactation. However, it can apply to younger women following premature ovarian failure or premature menopause. Unscheduled bleeding in women of menopausal age taking hormone replacement therapy (HRT) should be managed in the same way from a practical perspective.[2] 'Unscheduled bleeding' is defined as non-cyclical bleeding still continuing six months after commencing HRT or after six months of amenorrhoea.

Watch that video of a Man's Arm Exploded Due to Illegal Muscles Injections
