- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Open heart (coronary artery bypass, or CABG) surgery is performed in order to reroute, or "bypass," blood around blocked arteries, thereby improving the supply of oxygen-rich blood to the heart. Surgeons usually use an artery from the chest wall to construct the "detour" around the blocked part of the artery. Veins from the legs are also used.

nkylosing spondylitis (pronounced ank-kih-low-sing spon-dill-eye-tiss), or AS, is a form of arthritis that primarily affects the spine, although other joints can become involved. It causes inflammation of the spinal joints (vertebrae) that can lead to severe, chronic pain and discomfort

Total Contact Casting is the gold standard for treating diabetic foot ulcers; it's the most evidence-based treatment available. The Wound Care team at IU Health Methodist Hospital provides custom Total Contact Casting that completely offloads the wound, allowing it to heal in a matter of weeks.

In as many as 80% of cases, doctors don’t find the exact reason for a curved spine. Scoliosis without a known cause is what doctors call “idiopathic.” Some kinds of scoliosis do have clear causes. Doctors divide those curves into two types -- structural and nonstructural. In nonstructural scoliosis, the spine works normally, but looks curved. Why does this happen? There are a number of reasons, such as one leg’s being longer than the other, muscle spasms, and inflammations like appendicitis. When these problems are treated, this type of scoliosis often goes away.

The operation of vasectomy

Fetal heart sound by sonique
Lichen sclerosus is a skin condition that mainly affects the genital skin (vulva) in women and the penis in men. It most commonly occurs in middle-aged women. Symptoms may include itch, soreness, and changes in the appearance of affected skin.

The removal of a clot is called an embolectomy. An embolectomy might be done during a surgery. Or it might be done with a minimally invasive procedure that uses a catheter (a thin tube that is guided through a blood vessel). This type of treatment for pulmonary embolism is used only in rare cases.
ormal sperm densities range from 15 million to greater than 200 million sperm per milliliter of semen. You are considered to have a low sperm count if you have fewer than 15 million sperm per milliliter or less than 39 million sperm total per ejaculate.
Vaginal Hysterectomy Procedure of a 42 years old female patient with a 3 months history of symptomatic vaginal bulge

Bartholin gland Marsupialization in Primary Bartholin Cyst
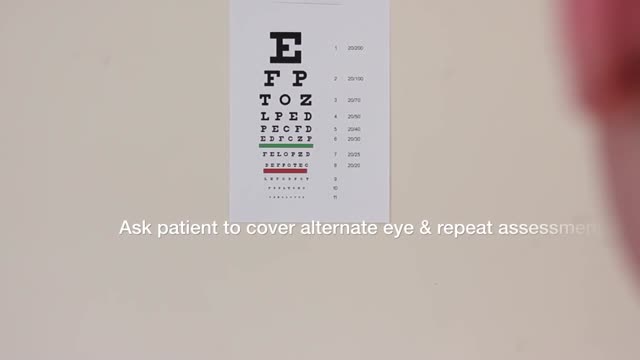
Examination of the Eyes and Vision
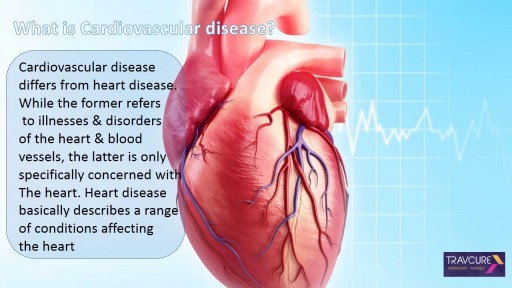
Cardiovascular surgery basically treats a number of diseases and medical disorders that affect your heart and the network of arteries and veins connecting it to every part of the body. https://goo.gl/iphEi9
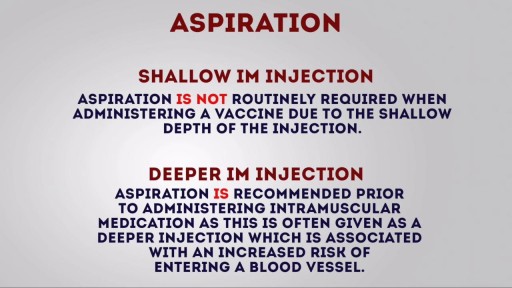
Intramuscular (IM) injection Tutorial for Nurses Video

A video showing surgery for hydrocele

Bleeding from Duodenal Ulcer

Loyola Respiratory System Exam Part 2 A video from Loyola Medical School, Chicago showing the medical and clinical examination of the respiratory system.

At URBN Dental, we provide you with top oral hygiene tips to help keep your mouth clean, healthy, and happy. Your manual toothbrush usually comes equipped with a tongue cleaner on the back of its head. That can be helpful in scrubbing your tongue, or you can also use a tongue cleaner. By using simple forward motions on the tongue, you can rid the area of plaque and bacteria which often cause bad breath, gingivitis, and harmful mouth ulcers.
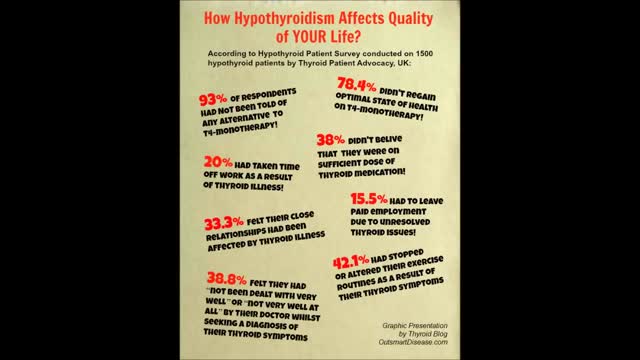
Through the hormones it produces, the thyroid gland influences almost all of the metabolic processes in your body. Thyroid disorders can range from a small, harmless goiter (enlarged gland) that needs no treatment to life-threatening cancer. The most common thyroid problems involve abnormal production of thyroid hormones. Too much thyroid hormone results in a condition known as hyperthyroidism. Insufficient hormone production leads to hypothyroidism. Although the effects can be unpleasant or uncomfortable, most thyroid problems can be managed well if properly diagnosed and treated.
Immune Responses During a Lupus Flare Video
