- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
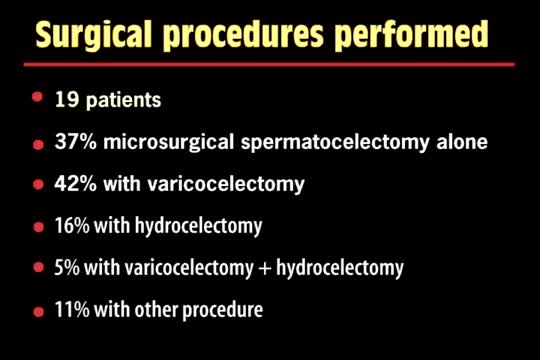
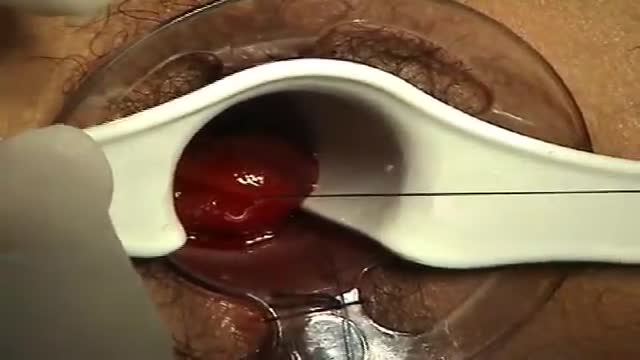
A spermatocelectomy is surgery to remove a spermatocele. A spermatocele is a cyst (sac of fluid) that contains sperm. It forms inside your scrotum on the outside of your testicle. The cyst is most often attached to your epididymis. The epididymis is a tube that stores sperm.

Panic attack from Injection:'(

Pediatrics abdominal examination

Having surgery can be frightening for anyone, but it's especially scary for kids who don't always understand what's going on, or what the grown-ups are saying. We're here to help!
Join Avrie, who had surgery at the Sacred Heart Children's Hospital pediatric surgery center in Spokane, WA. Maybe after watching and hearing her story, you and your kiddo will feel better about having surgery in the hospital.
Follow Avrie's trip - from check-in, vital signs and pre-op checks; meeting the doctor who will do his surgery, along with the anesthesiologist, surgery nurse and the Child Life Specialist; the trip to the Operating Room; waking up in the recovery room with his mom by his side; and getting ready to go home.
To learn more about the pediatric surgery center at Sacred Heart Children's Hospital, visit https://washington.providence.....org/locations-direct

Guest: Dr. Vicente Santos Jr., Ophthalmologist/President - Fatima University Medical Center
Date Aired: August 14, 2015
Visit http://www.untvweb.com/programs/good-morning-kuya
Sanjeev Dutta, MD, FACS discusses the fascinating new world of surgical technology. The pediatric general surgeon shares how medicine and technology have combined to achieve less invasive procedures and healthier outcomes for surgical patients.
Dr. Dutta is a pediatric general surgeon at Lucile Packard Children's Hospital. He is also an Associate Professor of Surgery at Stanford School of Medicine and Surgical Director of the Multidisciplinary Initiative for Surgical Technology Research.
Learn more about Stanford Children's Health. http://www.stanfordchildrens.org.

Most condoms are made of latex rubber, but they can also be made from lamb cecum or polyurethane. In addition to their contraceptive value, condom use has been found effective in preventing the spread of sexually transmitted diseases.

Will you still love me if I have herpes? About 1 in 6 Americans between the ages of 14 and 49 is infected with herpes simplex virus type 2, according to a health survey released by the Centers for Disease Control and Prevention. If you’re living with herpes, HSV, HPV or other STDs, you're recommended to check out the largest STD support site STDdatings.

Excision of Pilonidal Cyst. Open method.
A surgeon begins the PPH stapled hemorrhoidectomy by inserting a circular anal dilator and obturator into the anal canal and then securing the dilator in place with four sutures. The surgeon then inserts a PPH anoscope into the obturator. Next, he places a circumferential purse-string suture of 2-0 Monocryl on a UR-6 needle 4 cm proximal to the dentate line. The surgeon opens a PPH stapler and places its anvil across the purse string. The stapler is then closed and fired; it is held closed for two minutes to improve hemostasis. Prior to firing the stapler in a female patient, the surgeon places a gloved finger in the vagina to ensure the vaginal mucosa and rectal-vaginal septum are not trapped within the jaws of the closed stapler. The surgeon then opens and removes the stapler.

In this video, Jenna talks about Braxton Hicks contractions and preparing for labor.
plantar fasciitis and calcaneal spur can be treated by EPFR with calcanean drilling - endoscopic plantar fascia release علاج الشوكة العظمية للكعب بالمنظار د. أسامة الشاذلي مدرس جراحة العظام واستشاري جراحات و مناظير القدم والكاحل كلية الطب جامعة عين شمس

Ingrown Hair Removal Video
Surprising Facts About High Blood PressureMust

Open Appendectomy Surgery Video
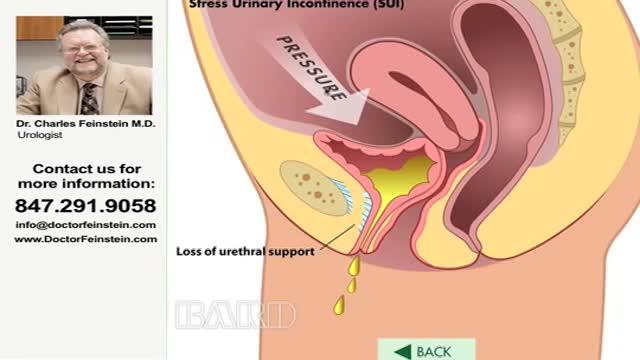
Urinary incontinence — the loss of bladder control — is a common and often embarrassing problem. The severity ranges from occasionally leaking urine when you cough or sneeze to having an urge to urinate that's so sudden and strong you don't get to a toilet in time. If urinary incontinence affects your daily activities, don't hesitate to see your doctor. For most people, simple lifestyle changes or medical treatment can ease discomfort or stop urinary incontinence
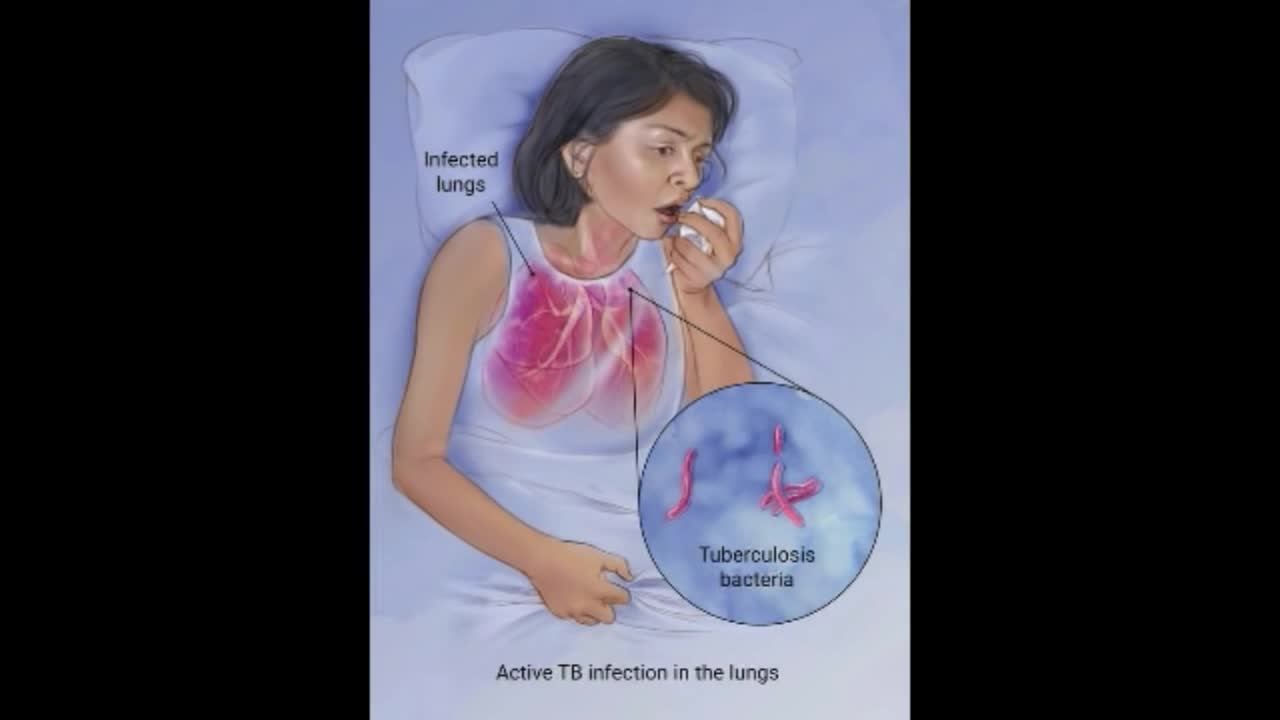
Although your body may harbor the bacteria that cause tuberculosis, your immune system usually can prevent you from becoming sick. For this reason, doctors make a distinction between: Latent TB. In this condition, you have a TB infection, but the bacteria remain in your body in an inactive state and cause no symptoms. Latent TB, also called inactive TB or TB infection, isn't contagious. It can turn into active TB, so treatment is important for the person with latent TB and to help control the spread of TB. An estimated 2 billion people have latent TB. Active TB. This condition makes you sick and can spread to others. It can occur in the first few weeks after infection with the TB bacteria, or it might occur years later. Signs and symptoms of active TB include: Coughing that lasts three or more weeks Coughing up blood Chest pain, or pain with breathing or coughing Unintentional weight loss Fatigue Fever Night sweats

Colorectal surgeon Conor Delaney, MD, explains laparoscopic surgery for colon cancer, including how it works and what patients can typically expect before, during, and after the procedure.
Learn more about colon cancer at http://cancer.org/coloncancer

Barrett's esophagus is a complication of chronic (long lasting) and usually severe gastrointestinal reflux disease (GERD), but occurs in only a small percentage of patients with GERD. Criteria are needed for screening patients with GERD for Barrett's esophagus. Until validated criteria are available, it seems reasonable to do screening endoscopies in GERD patients who cannot be taken off acid suppression therapy after two to three years. The diagnosis of Barrett's esophagus rests upon seeing (at endoscopy) a pink esophageal lining that extends a short distance (usually less than 2.5 inches) up the esophagus from the gastroesophageal junction and finding intestinal type cells (goblet cells) on biopsy of the lining. There is a small but definite increased risk of cancer of the esophagus (adenocarcinoma) in patients with Barrett's esophagus.

Testis operation
