- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
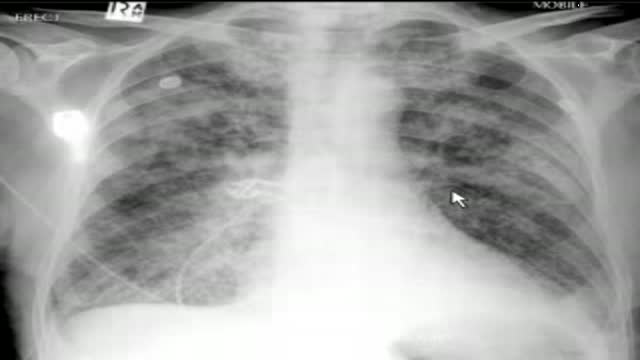
The video will describe pulmonary edema. Please see disclaimer on my website. www.academyofprofessionals.com
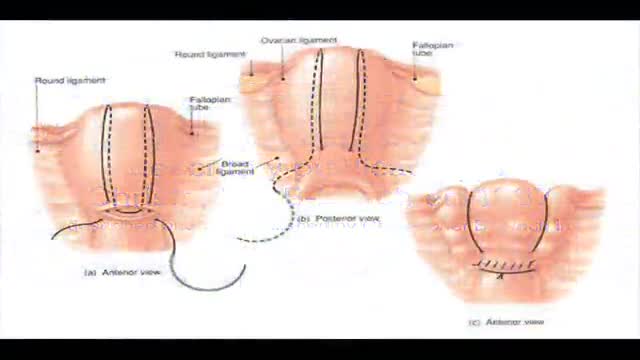
B-Lynch suture for uterine atony technique described
Video is an excellent introduction to Hysterosalpingography and summarizes different pathologies. While the information on this presentation is about health care issues, it is not medical advice. People seeking specific medical advice or assistance should contact their personal physician. Although we believe the information in this presentation to be accurate and timely, because of the rapid advances in health care and our reliance on information provided by outside sources, we make no warranty or guarantee concerning the accuracy or reliability of the content or other material which we may reference. When clinical matters are discussed, the opinions presented are those of the discussants only. The material discussed on the presentation is not intended to present the only or necessarily the best method or procedure, but rather presents the approach or opinion of the discussant. This presentation is provided in an “as is” format without warranties of any kind, expressed or implied, including but not limited to warranties of title, non-infringement or implied warranties of merchantability or fitness for a particular purpose.
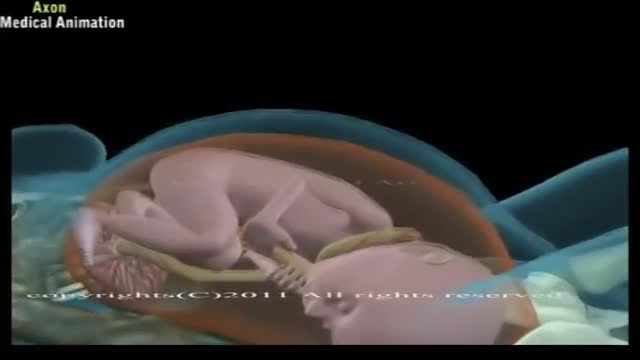
A cesarean delivery is a surgical procedure in which a fetus is delivered through an incision in the mother's abdomen and uterus. ... According to the CDC, in 2010, almost 33% of births were by cesarean delivery.

An appendectomy (sometimes called appendisectomy or appendicectomy) is the surgical removal of the vermiform appendix. This procedure is normally performed as an emergency procedure, when the patient is suffering from acute appendicitis.

Off-Pump Coronary Artery Bypass Grafting (CABG)

The HEENT, or Head, Eye, Ear, Nose and Throat Exam is usually the initial part of a general physical exam, after the vital signs. Like other parts of the physical exam, it begins with inspection, and then proceeds to palpation. It requires the use of several special instruments in order to inspect the eyes and ears, and special techniques to assess their special sensory function. This module reviews some of the relevant surface anatomy and describes the basic HEENT exam. The module includes an introduction to use of the ophthalmoscope.

Suprapubic Catheterization / Cystostomy

Surgical removal of a Chalazion from the eye lid

6 987 24 MORE How Does Anesthesia Work? Credit: itsmejust | Shutterstock If you’ve ever had surgery, unless you are super tough, you’ve gone through it with the benefit of anesthetics. But, how do these body-numbing elixirs work? Prior to the invention of anesthesia in the mid-1800s, surgeons had to hack off limbs, sew up wounds and remove mysterious growths with nothing to dull the patient's pain but opium or booze. While these drugs may have numbed the patient, they didn’t always completely block the pain, or erase the memory of it. Since then, doctors have gotten much better at putting us out with drug combinations that ease pain, relax muscles and, in some cases, put us in a deep state of hypnosis that gives us temporary amnesia. Today, there are two primary types of anesthesia drugs: those that knockout the whole body (general) and those that only numb things up locally.

How to obtain a blood sample
Watch that video to know How to Increase Your Chances of Getting Pregnant?
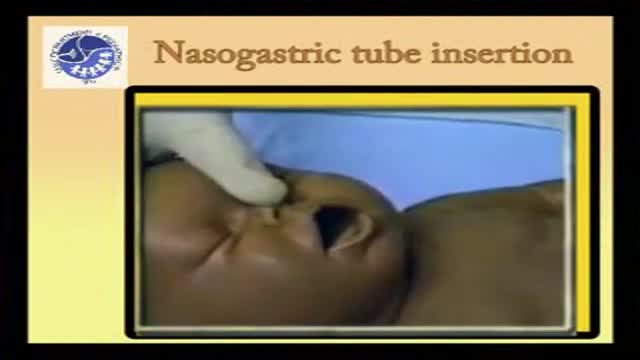
Insertion of pediatric nasogastric tube in children and babies

Watch that video of a v

Full complete clinical examination of the chest, lungs and respiration with breath sounds

Watch that Fishing Hook Inside Eye Removal Surgery
The menstrual cycle is the regular natural change that occurs in the female reproductive system like the uterus and ovaries that make pregnancy possible. The cycle is required for the production of ovocytes, and for the preparation of the uterus for pregnancy.
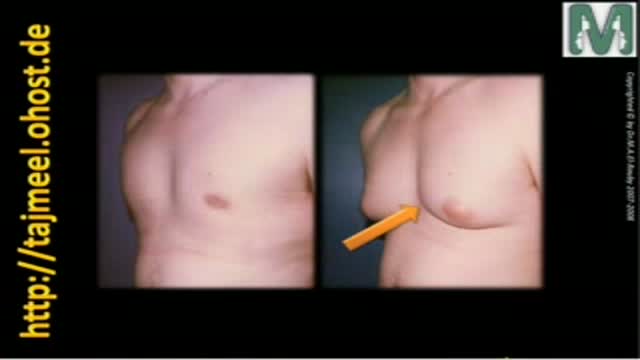
Gynecomastia means enlargement of male breast to resample female breast that is a common problem between males and causes many psychological problem
Dr. Mohamed El-Rouby
Consltant of Plastic surgery - Faculty of Medicine - Ain Shams University
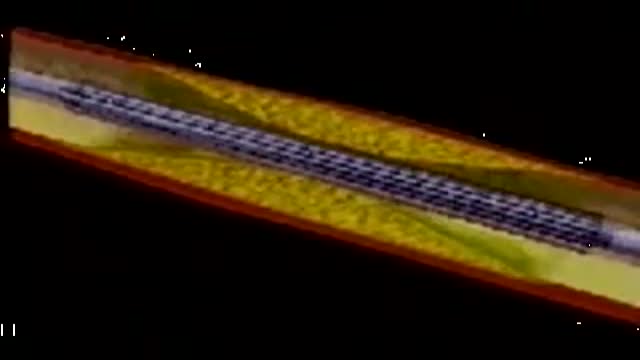
This video depicts how a stent is placed in the coronary artieries. We first place a guiding wire in the heart artery through a catheter, usually from the groin. Then the stent is inflated by a balloon in the artery, which is then removed. The stent remains permanently. Blood thinners, aspirin and plavix, are both required after a stent is placed in your heart artery.
