- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Inflammation of the uvula is known as uvulitis. Your uvula will appear red, puffy, and larger than normal. Other symptoms of uvulitis may include: itching burning a sore throat spots on your throat snoring difficulty swallowing trouble breathing If you have a swollen uvula along with a fever or abdominal pain, consult with your doctor right away. In rare cases, the uvula can swell enough to block your airway. Swelling of the throat is a life-threatening event. If this happens, seek immediate medical attention. What causes a swollen uvula? Causes Inflammation is your body’s response when it’s under attack. Triggers for inflammation include: environmental and lifestyle factors an infection trauma genetics Environmental and Lifestyle Factors The most common food allergies are peanuts tree nuts milk eggs wheat soy fish, including shellfish You could be having an allergic reaction to something you touched, swallowed, or breathed in. Some common allergens include: food irritants , such as dust, animal dander, or pollen medication exposure to chemicals or other toxic substances, including tobacco Infection You can get viral infections or bacterial infections. Examples of viral infections include: the common cold the flu mononucleosis chickenpox measles croup The most common bacterial infection is strep throat, which occurs due to Streptococcus pyogenes, which is a type of group A Streptococcus. If you have infected tonsils, or tonsillitis, severe inflammation can cause them to push against and irritate your uvula. Trauma Trauma to the uvula can happen if you need an intubation, such as during surgery. Your uvula can also be injured during a tonsillectomy. This is a procedure to remove your tonsils, which are located on both sides of your uvula. Your throat and uvula can also become irritated if you have acid reflux disease or if you vomit frequently. Genetics A condition called hereditary angioedema (HAE) can cause swelling of the uvula and throat, as well as swelling of the face, hands, and feet. Other symptoms include nausea, vomiting, and abdominal pain. It’s an uncommon genetic mutation that occurs in 1 in 10,000 to 1 in 50,000 people. It’s rare, but there are case reports of individuals who have an elongated uvula, which can also interfere with breathing. What are the risk factors for a swollen uvula? Risk Factors Anyone can get uvulitis, but adults get it less often than children do. You’re at increased risk if you: have allergies use tobacco products are exposed to chemicals and other irritants in the environment have a weakened immune system, making you more susceptible to infections How is a swollen uvula diagnosed? Diagnosis If you have fever or swelling of your throat, see your doctor. Be prepared to give a complete medical history. Tell your doctor: about all the over-the-counter and prescription medications you take if you’re a smoker or you chew tobacco if you’ve recently tried new foods if you’ve been exposed to chemicals or unusual substances about your other symptoms, such as abdominal pain, fever, or dehydration Your doctor may be able to make a diagnosis through a physical exam. It’s likely you’ll also need a throat swab to evaluate for strep or to obtain secretions for culture to determine if you have another bacterial or fungal infection. This test is known as the rapid strep test. You may also need a nasal swab to test for influenza. Blood testing can help identify or rule out some other infectious agents. If those tests are inconclusive, you may need to see an allergist. Blood and skin tests can help identify foods or other substances that cause a reaction. Learn more: Allergy testing » If necessary, imaging tests can provide a more detailed view of your throat and the surrounding area. What’s the treatment for a swollen uvula? Treatment When you have something like the common cold, swelling usually clears up on its own without treatment. Otherwise, treatment will depend on how severe your symptoms are, as well as what’s causing the inflammation. Infection Viral infections tend to clear up without treatment. The only upper respiratory infection for which an antiviral medication is available is influenza. Antibiotics can treat bacterial infections. Even after symptoms clear up, take all the medication as prescribed. If your condition may be contagious, stay home until your doctor tells you that you’re no longer at risk of spreading it to others. Allergy If you test positive for an allergy, try to avoid the allergen in the future. Doctors usually treat allergies with antihistamines or steroids. Anaphylaxis is a severe allergic reaction. Doctors use epinephrine to treat this reaction. Hereditary angioedema Your doctor may treat HAE with any of the following: anabolic steroids, or androgens antifibrinolytics C1 inhibitors, such as C1 esterase inhibitor (Berinert) or C1 esterase inhibitor (recombinant) (Ruconest) a plasma kallikrein inhibitor, such as ecallantide (Kalbitor) bradykinin receptor antagonist, such as icatibant injection (Firazyr) Tell your doctor if you have new or worsening symptoms, and follow up as necessary. Tips for relief home treatment If you have a swollen uvula or sore throat, it’s your body’s way of telling you that something is wrong. A few home remedies can help keep you strong and soothe your irritated throat. Make sure you’re getting enough fluids. If your throat hurts when you drink, try drinking small amounts throughout the day. Your urine should be light in color. If it’s dark yellow or brown, you’re not drinking enough and may be dehydrated. Additional tips include the following: Cool your throat by sucking on ice chips. Frozen juice bars or ice cream may also do the trick. Gargle with warm salt water to ease your dry, scratchy throat. Aim for a full night’s sleep, and nap during the day if you can. What’s the outlook? Outlook A swollen uvula isn’t a common occurrence. Most of the time it clears up without treatment. If you have an infection, prompt treatment should take care of the problem within a week or two. If you have allergies that lead to swelling of the uvula or throat, do your best to avoid that allergen. You should also be prepared to deal with an attack if you come into contact with the substance again. If you’ve ever had anaphylaxis, ask your doctor if you should carry injectable epinephrine (EpiPen) in case of emergency. People with HAE must learn to recognize triggers and early warning signs of an attack. Talk to your doctor about how to manage HAE. Article Resources Was this article helpful?Yes No Share Tweet Email Print Read This Next 9-Month-Old Baby: Developmental Milestones and Guidelines 9-Month-Old Baby: Developmental Milestones and Guidelines Read More » All of the ‘Firsts’ That Come with Breast-Feeding All of the ‘Firsts’ That Come with Breast-Feeding Read More » 5 Types of Health Professionals You Should Know About 5 Types of Health Professionals You Should Know About Read More » What’s the Difference Between a Fracture and a Break? What’s the Difference Between a Fracture and a Break? Read More » Is Corn a Vegetable? Is Corn a Vegetable? Read More » Advertisement Advertisement Advertisement

Your temporomandibular joint is a hinge that connects your jaw to the temporal bones of your skull, which are in front of each ear. It lets you move your jaw up and down and side to side, so you can talk, chew, and yawn. Problems with your jaw and the muscles in your face that control it are known as temporomandibular disorders (TMD). But you may hear it wrongly called TMJ, after the joint.

Most condoms are made of latex rubber, but they can also be made from lamb cecum or polyurethane. In addition to their contraceptive value, condom use has been found effective in preventing the spread of sexually transmitted diseases.

Pancreatic cysts are saclike pockets of fluid on or in your pancreas, a large organ behind the stomach that produces hormones and enzymes that help digest food. Most pancreatic cysts aren't cancerous, and many don't cause symptoms. They're typically found during imaging testing for another problem. Some are actually noncancerous (benign) pockets of fluids lined with scar or inflammatory tissue, not the type of cells found in true cysts (pseudocysts). But some pancreatic cysts can be or can become cancerous. Your doctor might take a sample of the pancreatic cyst fluid to determine if cancer cells are present. Or your doctor might recommend monitoring a cyst over time for changes that indicate cancer.

Open Appendectomy Surgery Video
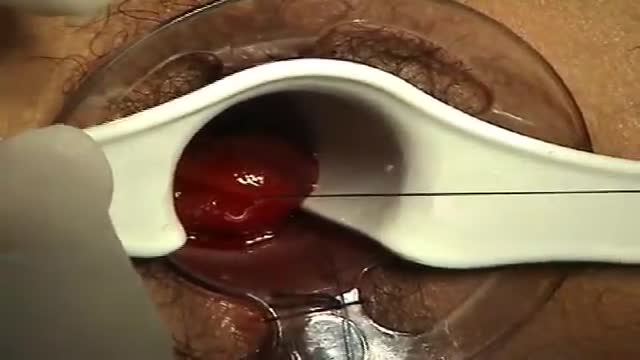
A surgeon begins the PPH stapled hemorrhoidectomy by inserting a circular anal dilator and obturator into the anal canal and then securing the dilator in place with four sutures. The surgeon then inserts a PPH anoscope into the obturator. Next, he places a circumferential purse-string suture of 2-0 Monocryl on a UR-6 needle 4 cm proximal to the dentate line. The surgeon opens a PPH stapler and places its anvil across the purse string. The stapler is then closed and fired; it is held closed for two minutes to improve hemostasis. Prior to firing the stapler in a female patient, the surgeon places a gloved finger in the vagina to ensure the vaginal mucosa and rectal-vaginal septum are not trapped within the jaws of the closed stapler. The surgeon then opens and removes the stapler.

Transmetatarsal Amputation for Gangrene

Furosemide is used to reduce extra fluid in the body (edema) caused by conditions such as heart failure, liver disease, and kidney disease. This can lessen symptoms such as shortness of breath and swelling in your arms, legs, and abdomen. This drug is also used to treat high blood pressure. Lowering high blood pressure helps prevent strokes, heart attacks, and kidney problems. Furosemide is a "water pill" (diuretic) that causes you to make more urine. This helps your body get rid of extra water and salt.

examination of a case of inguino-scrotal swelling as in cases of oblique inguinal hernia..etc
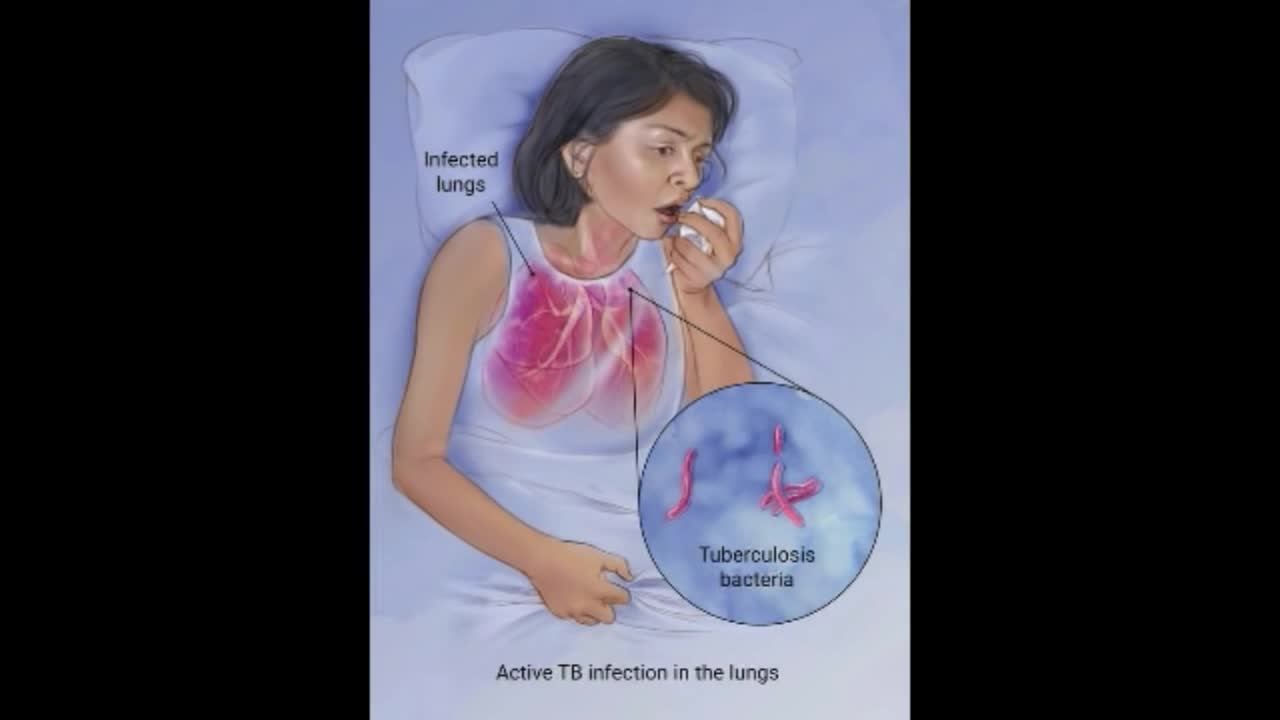
Although your body may harbor the bacteria that cause tuberculosis, your immune system usually can prevent you from becoming sick. For this reason, doctors make a distinction between: Latent TB. In this condition, you have a TB infection, but the bacteria remain in your body in an inactive state and cause no symptoms. Latent TB, also called inactive TB or TB infection, isn't contagious. It can turn into active TB, so treatment is important for the person with latent TB and to help control the spread of TB. An estimated 2 billion people have latent TB. Active TB. This condition makes you sick and can spread to others. It can occur in the first few weeks after infection with the TB bacteria, or it might occur years later. Signs and symptoms of active TB include: Coughing that lasts three or more weeks Coughing up blood Chest pain, or pain with breathing or coughing Unintentional weight loss Fatigue Fever Night sweats

Having surgery can be frightening for anyone, but it's especially scary for kids who don't always understand what's going on, or what the grown-ups are saying. We're here to help!
Join Avrie, who had surgery at the Sacred Heart Children's Hospital pediatric surgery center in Spokane, WA. Maybe after watching and hearing her story, you and your kiddo will feel better about having surgery in the hospital.
Follow Avrie's trip - from check-in, vital signs and pre-op checks; meeting the doctor who will do his surgery, along with the anesthesiologist, surgery nurse and the Child Life Specialist; the trip to the Operating Room; waking up in the recovery room with his mom by his side; and getting ready to go home.
To learn more about the pediatric surgery center at Sacred Heart Children's Hospital, visit https://washington.providence.....org/locations-direct

https://bit.ly/3HIStRc #shorts
Tracheotomy and tracheostomy are surgical procedures that create an opening in the trachea (windpipe) to help patients breathe when they have difficulty doing so through the nose or mouth. Though they are similar in purpose, there are some key differences between them.
Tracheotomy is a temporary procedure that involves creating a small incision in the trachea to insert a breathing tube. The tube is typically removed once the patient no longer requires it, and the incision heals on its own. Tracheostomy, on the other hand, is a more permanent solution that involves creating a hole in the trachea and inserting a tracheostomy tube, which remains in place for an extended period.
Indications for these procedures include:
Airway obstruction due to trauma, tumors, or infection
Severe respiratory distress or failure
Prolonged mechanical ventilation
Inability to protect the airway due to neurological disorders or impaired consciousness
Steps for performing a tracheotomy and tracheostomy:
Preparation: The patient is positioned, and the neck area is cleaned and draped. Local anesthesia is often administered, although general anesthesia may be used in some cases.
Incision: A small incision is made in the neck, and the muscles and tissues are carefully separated to expose the trachea.
Tracheal opening: A small opening is made in the trachea, typically between the second and third tracheal rings.
Tube insertion: A tracheotomy tube is inserted through the incision and into the trachea for a tracheotomy, while a tracheostomy tube is inserted for a tracheostomy. Both tubes are secured in place.
Confirmation: Proper placement of the tube is confirmed by listening for breath sounds and checking for adequate ventilation.
Pre-operative care typically involves a thorough assessment of the patient's medical history, as well as any necessary imaging studies or lab tests to ensure the procedure is appropriate and safe. Informed consent should be obtained from the patient or their legal representative.
Post-operative care includes monitoring the patient's vital signs, ensuring the tube remains secure and patent, and managing any pain or discomfort. For tracheostomy patients, regular cleaning and maintenance of the stoma (the opening in the trachea) and the tracheostomy tube are essential to prevent infection and other complications. Long-term care may involve speech therapy, respiratory therapy, and support from a multidisciplinary team to address any ongoing needs.
It's crucial to remember that these procedures should only be performed by trained medical professionals in a clinical setting.
for additional information about this procedure check our article @ www.medicalartsshop.com
For more free resources, find us on Pinterest & Facebook pages:
https://www.pinterest.ca/medicalartsofficial/
https://www.facebook.com/Medicalartsofficial
https://www.youtube.com/@medic....alarts?sub_confirmat
https://www.instagram.com/medicalartsofficial/
https://www.tiktok.com/@medicalarts
This video and associated content are for entertainment and educational purposes only!!

Dr. Lohith U, Consultant Surgical Gastroenterology, Bariatric and GI Oncology, Manipal Hospital Sarjapur, speaks about advanced laparoscopic surgery in this informative video. He shares details about the procedure,insights on its advantages, and how it can help treat gastrointestinal issues without making large incisions in a patient’s body. To know more watch this video.
Consult the experts here - https://bit.ly/3RiWqPr
#ManipalHospitalSarjapur #YourManipal #LifesOn #Healthcare #LaparoscopicSurgery
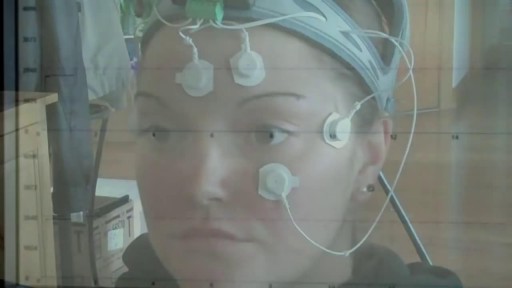
Electronystagmography (ENG) is a diagnostic test to record involuntary movements of the eye caused by a condition known as nystagmus. It can also be used to diagnose the cause of vertigo, dizziness or balance dysfunction by testing the vestibular system.

A video showing insertion of a percutaneous endoscopic colostomy in a frail patient with recurrent sigmoid volvulus.

This video clip shows nasolabial cyst being excised under local anesthesia

Diabetic neuropathy is a type of nerve damage that can occur if you have diabetes. High blood sugar (glucose) can injure nerve fibers throughout your body, but diabetic neuropathy most often damages nerves in your legs and feet. Depending on the affected nerves, symptoms of diabetic neuropathy can range from pain and numbness in your extremities to problems with your digestive system, urinary tract, blood vessels and heart. For some people, these symptoms are mild; for others, diabetic neuropathy can be painful, disabling and even fatal. Diabetic neuropathy is a common serious complication of diabetes. Yet you can often prevent diabetic neuropathy or slow its progress with tight blood sugar control and a healthy lifestyle.

Generic minoxidil is known to treat hair-fall issues in men and women, it is best for hair growth, hair re-development, etc. it is available in the strength of 5mg and easily available at online pharmacy store. For more information visit to http://www.medstorerx.com/generic-minoxidil.aspx
Arterial Blood Gas Sampling

If you notice a patient beginning to fall, follow these steps to help lower them safely to floor. Always stay with the patient and call for additional help.
Download the CNA Mastery app: https://onelink.to/cnamastery
Download the My Mastery nursing app: https://mynursingmastery.com/get-started
