- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Bleeding from Duodenal Ulcer

Loyola Respiratory System Exam Part 2 A video from Loyola Medical School, Chicago showing the medical and clinical examination of the respiratory system.

Testicle pain (testicular pain) is pain that occurs in or around one or both testicles. Sometimes testicle pain actually originates from somewhere else in the groin or abdomen, and is felt in one or both testicles (referred pain).
Immune Responses During a Lupus Flare Video

Stop suffering alone and get relief from vaginal atrophy symptoms

Always consult your doctor and seek help early enough to prevent complications

What are the disadvantages of male condoms? a moderately high failure rate when used improperly or inconsistently. the potential for diminished sensation. skin irritation, such as contact dermatitis, due to latex sensitivity or allergy. allergic reactions to spermicides, lubes, scents, and other chemicals in the condoms.
Testicular Self Exam
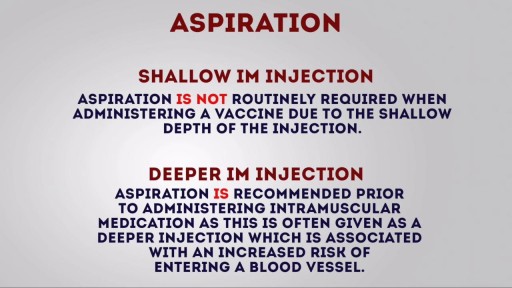
Intramuscular (IM) injection Tutorial for Nurses Video

Infected Hernia Mesh Repair Surgery Video

In as many as 80% of cases, doctors don’t find the exact reason for a curved spine. Scoliosis without a known cause is what doctors call “idiopathic.” Some kinds of scoliosis do have clear causes. Doctors divide those curves into two types -- structural and nonstructural. In nonstructural scoliosis, the spine works normally, but looks curved. Why does this happen? There are a number of reasons, such as one leg’s being longer than the other, muscle spasms, and inflammations like appendicitis. When these problems are treated, this type of scoliosis often goes away.
Cardiovascular surgery basically treats a number of diseases and medical disorders that affect your heart and the network of arteries and veins connecting it to every part of the body. https://goo.gl/iphEi9

Demonstrates some of the procedures of the Cardio Vascular / Peripheral Vascular exam.
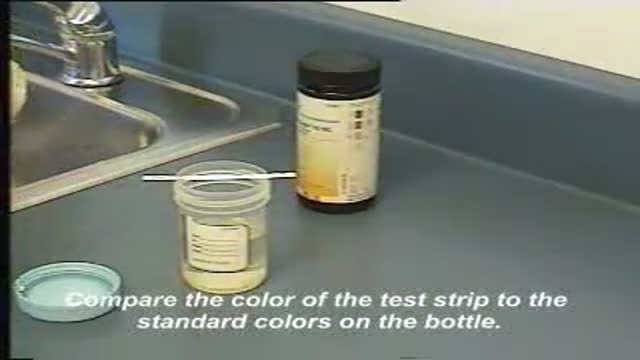
This video demonstrates how use a commercially-prepared "dip-stick" to test a random urine specimen for the presence of protein or glucose.

To learn more about licensing this video for content marketing or patient education purposes, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=stroke-071411
This video, created by Nucleus Medical Media, gives a thorough explanation of stroke, covering anatomy and physiology, different types of stroke, and treatment.
ANH11048

Wetness. Even the most absorbent diaper leaves some moisture on your child's skin. And when your child's urine mixes with bacteria from his stool, it breaks down into ammonia, which can be very harsh on the skin. That's why children with frequent bowel movements or diarrhea are more prone to diaper rash.

Fractured implant extraction

Patient 65-year-old of age who comes to the medical consultation with pain moderated pain in the right hypochondrium of “several years of evolution” but that it increased one week ago. Also, she shows pain in the umbilical region of “many years of evolution”, that is supported according to the patient - in a constant way.rnTo the examination, we observe an umbilical hernia, apparently divided into two parts. The hernia of the external region measures 25.1 centimeters x 18.0 centimeters and the one that occupies the average region measures 12.0 centimeters x 10.0 centimeters.rnPatient who comes to the medical consultation with moderated pain in the right hypochondrium of one year of evolution but it increased one week ago after eat duck.rnIn the ultrasound scan of the region of the right hypochondrium (patient came having breakfast, that is to say, without previous preparation ) we can observe the liver of 123.8 millimeters high, as well as the porta vein with a diameter of 7.3 millimeters.rnOn having observed the Gallbladder, we think that a side wall is increased in 2.7 mm (hyperechogenic) with several “echogenics points” in the interior (”Biliary Mud”).
The measurements of the gallbladder were: 39.0 x 17.4 millimeters.rnWe can appreciates an echogenic image in the interior that it would make think about stone. The stones are identified as echogenic foci casting acoustic shadowing but but this image did not appear and a re-evaluation is decided in 15 days.
Acalculous cholecystopathy which means disease or condition of the gallbladder without the presence of gallstones. You might also call it functional gallbladder disorder or impaired gallbladder emptying. Some causes may be chronic inflammation, a problem with the smooth muscles of the gallbladder or the muscle of the Sphincter of Oddi being too tight.
REMEMBER:
Umbilical hernia is a congenital malformation, especially common in infants of African descent, and more frequent in boys. An Acquired umbilical hernia directly results from increased intra-abdominal pressure and are most commonly seen in obese individuals.
Presentation:A hernia is present at the site of the umbilicus (commonly called a navel, or belly button) in the newborn; although sometimes quite large, these hernias tend to resolve without any treatment by around the age of 5 years. Obstruction and strangulation of the hernia is rare because the underlying defect in the abdominal wall is larger than in an inguinal hernia of the newborn. The size of the base of the herniated tissued is inversely correlated with risk of strangulation (i.e. narrow base is more likely to strangulate).
Babies are prone to this malformation because of the process during fetal development by which the abdominal organs form outside the abdominal cavity, later returning into it through an opening which will become the umbilicus.
Differential diagnosisrnImportantly this type of hernia must be distinguished from a paraumbilical hernia which occurs in adults and involves a defect in the midline near to the umbilicus, and from omphalocele.
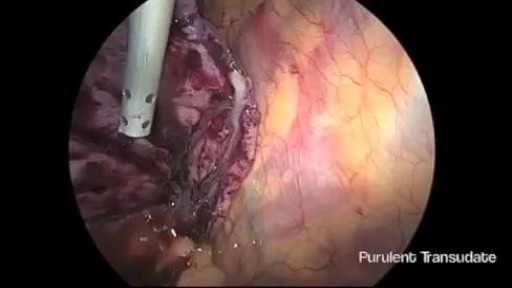
Thoracoscopic Management of Lung Abscess Before Empyema
