- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
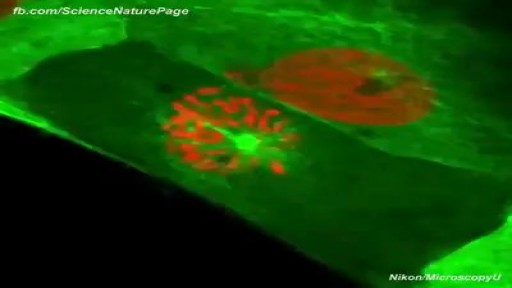
Actual Footage of Cell Division (Kidney Cells) see more http://www.kidneymy.com/

An amputation is the removal of an extremity or appendage from the body. Amputations in the upper extremity can occur as a result of trauma, or they can be performed in the treatment of congenital or acquired conditions. Although successful replantation represents a technical triumph to the surgeon, the patient's best interests should direct the treatment of amputations. The goals involved in the treatment of amputations of the upper extremity include the following : Preservation of functional length Durable coverage Preservation of useful sensibility Prevention of symptomatic neuromas Prevention of adjacent joint contractures Early return to work Early prosthetic fitting These goals apply differently to different levels of amputation. Treatment of amputations can be challenging and rewarding. It is imperative that the surgeon treat the patient with the ultimate goal of optimizing function and rehabilitation and not become absorbed in the enthusiasm of the technical challenge of the replantation, which could result in poorer outcome and greater financial cost due to lost wages, hospitalization, and therapy.
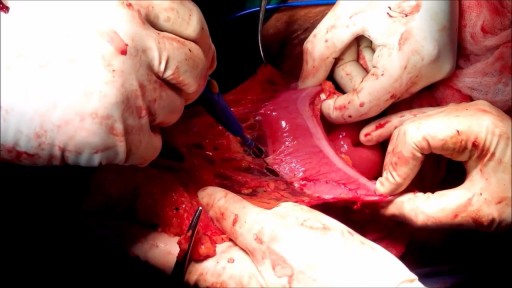
Mesenteric cyst is one of the rarest abdominal tumours, with approximately 820 cases reported since 1507. The incidence varies from 1 per 100,000 to 250,000 admissions. The lack of characteristic clinical features and radiological signs may present great diagnostic difficulties.

At URBN Dental, we provide you with top oral hygiene tips to help keep your mouth clean, healthy, and happy. Your manual toothbrush usually comes equipped with a tongue cleaner on the back of its head. That can be helpful in scrubbing your tongue, or you can also use a tongue cleaner. By using simple forward motions on the tongue, you can rid the area of plaque and bacteria which often cause bad breath, gingivitis, and harmful mouth ulcers.
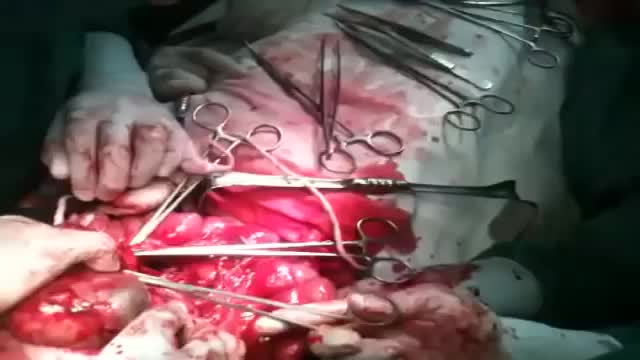
top 10 most incredible surgeries ever done
Digital Local Anaesthesia
An omentectomy is a surgical procedure designed to remove the omentum, which is a thin fold of abdominal tissue that encases the stomach, large intestine and other abdominal organs. This fatty lining contains lymph nodes, lymph vessels, nerves and blood vessels.

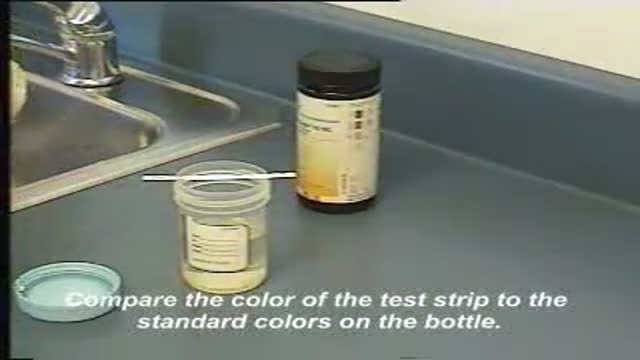
This video demonstrates how use a commercially-prepared "dip-stick" to test a random urine specimen for the presence of protein or glucose.
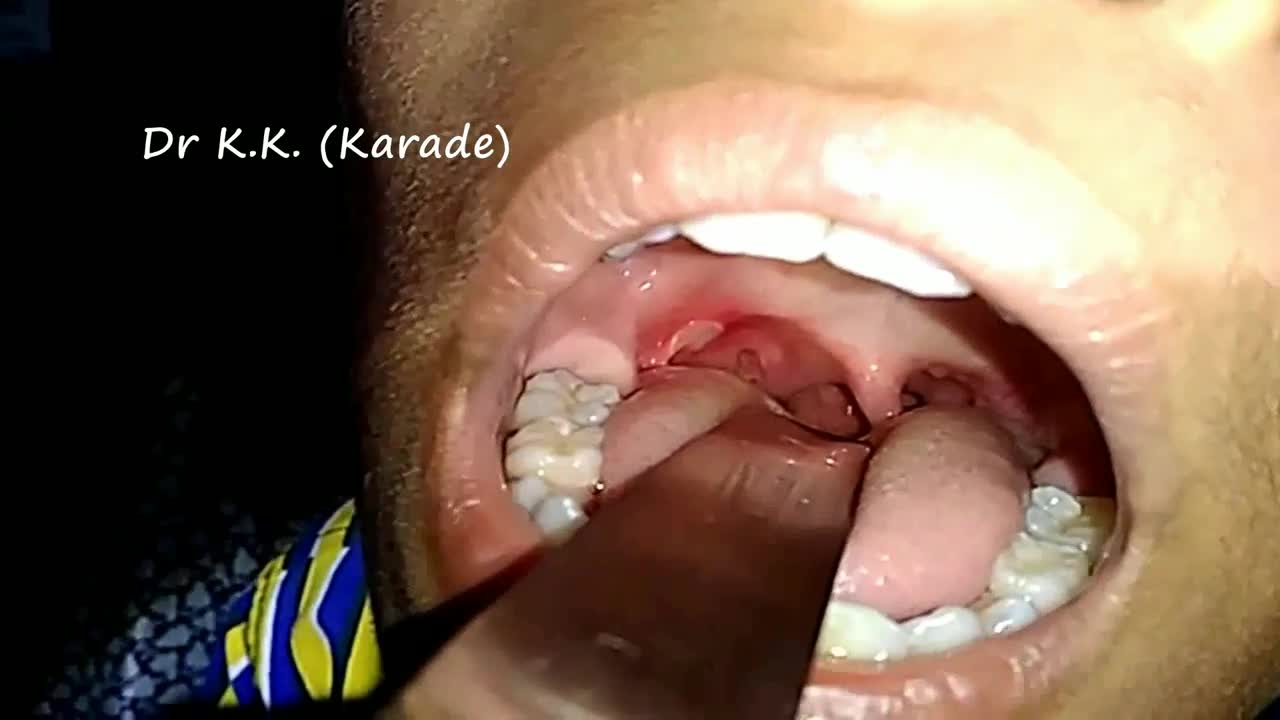
Canker sores (Aphthous ulcer) are small, painful ulcers on the inside of the mouth, tongue, lips, or throat.Canker sores are white or yellow and surrounded by a bright red area. They are not cancerous.

Large Breast Augmentation

Fractured implant extraction
USMLE Step 2 CS - DIARRHEA - This is just preview video. To get full access please visit our website : www.usmletutoring.com

Medication Through Running IV

10 Biggest Babies Ever Born

Nipple Sensation After Breast Augmentation
Time Management and Work Organization

Upper gastrointestinal bleeding (sometimes upper GI, UGI bleed, Upper gastrointestinal hemorrhage, gastrorrhagia) refers to bleeding in the upper gastrointestinal tract, commonly defined as bleeding arising from the esophagus, stomach, or duodenum. In fact, the proportion of UGIB cases caused by peptic ulcer disease has declined, a phenomenon that is believed to be due to the use of proton pump inhibitors (PPIs) and H pylori therapy. Duodenal ulcers are more common than gastric ulcers, but the incidence of bleeding is identical for both.

External cephalic version is a process by which a breech baby can sometimes be turned from buttocks or foot first to head first. External cephalic version (ECV) is a manual procedure that is advocated by national guidelines for breech presentation singleton pregnancy, in order to enable vaginal delivery.

DMC Eye specialist restores a woman's vision by removing cataracts and installing an artificial lens. ~ Detroit Medical Center
