- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Laparoscopic Uterosacral Colpoplexy HD
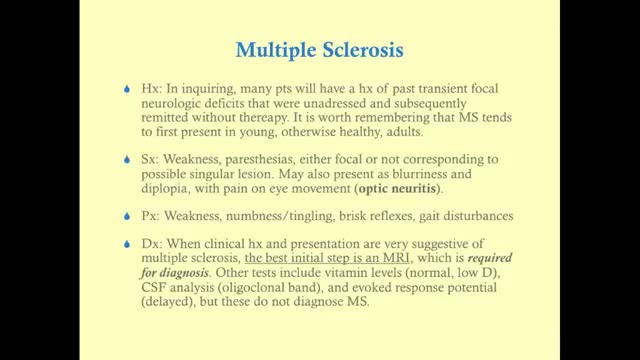
Multiple sclerosis (MS) affects the brain and spinal cord. Early MS symptoms include weakness, tingling, numbness, and blurred vision. Other signs are muscle stiffness, thinking problems, and urinary problems. Treatment can relieve MS symptoms and delay disease progression.
Time Management and Work Organization
Laparotomy Closure Abdomen Animation

Transcript: Body Restoration (http://stalbertphysiotherapy.com/) has treated over 12,400 patients since it opened its doors in 1992. While embracing new technology and techniques they have not left behind the basic tenets of hands-on healing. If you are injured or have chronic pain, the mission is to help you live pain-free. Relief is a click or a phone call away. Come in for your no obligation exam and find out what will work for you.
Pulsatile Tinnitus Cure, Constant Ear Ringing, Ear Wax Tinnitus, Whistling In Ear, Ringing In Ears. http://tinnitus-solution.info-pro.co First the good news - we know what causes tinnitus. And now the bad news - conventional medical science cannot cure it. Not permanently at least. Sure enough, your doctor would suggest a few remedies, and it may seem to you that the noises you hear are going down. As a result, you begin to relax believing that a pesky problem has been resolved. But suddenly the sounds return again. This is a very common problem actually. So let us turn to the causes instead, and see whether we can try to solve the issue from this end. Here Are Some of the Most Common Causes of Tinnitus Exposure to noise - Did your mom always tell you in your younger days to turn down the volume? She was right. Exposure to loud noise can give you tinnitus. In fact, rock musicians, and those who work with them, or in night clubs often have it. Those who work in construction sites also have tinnitus. So turn down that volume while you still can. You could begin to hear all kinds of noises if you have been exposed to just a single high-pitched noise. Or it could be due to a continuous attack of loud noises close to your ear. This is what happens. Prolonged exposure to noise can damage the Cochlea and cause tinnitus. So if you cannot simply stay away from all that noise, at least get some protection. Use an ear plug when you can. Head injury - Take care of your head because a severe blow or a slight bang could make you hear the tinnitus noises. The head is of course one of the most sensitive parts of the human body. But some people cannot live without an injury, such as those who are into sports - boxers and football players. That's why athletes are more prone to a tinnitus attack. Even a dental surgery could make you hear them. Ear infections and other ear problems - An ear infection, and even sinus can lead to tinnitus as well. When there is an allergy or a sinus infection, the mucous thickens within the inner ear, and this causes more pressure. The extra pressure can lead to tinnitus. Meniere's disease, where the fluid level goes up inside the middle ear is another reason. It could even cause hearing loss. Prescription medications - Conventional drugs often cause side effects, and tinnitus is one of them. Actually, all kinds of drugs have been blamed for instigating this condition. Such as antibiotics like Aminoglycosides, Erythromycin and Vancomycin, Aspirin or medicines containing it. Anti inflammatory drugs like Advil, Aleve, Anaprox, Clinoril, Feldene, Indocin, Lodine and Motrin have also been blamed. Sometimes people heard noises after taking chemotherapy agents such as Cisplatin, Nitrogen Mustard and Vincristine. And some others have even blamed quinine and loop diuretics for this. or even the result of a virus or infection. but is in fact far more shocking that you’ve been led to believe. You’ll finally be able to concentrate on your life, rather that the incessant noise. You’ll be able to no longer live in fear of loud noises, of music, of cinemas. of having fun. The Tinnitus Scandal Revealed, A cure DOES exist. click here: http://tinnitus-solution.info-pro.co

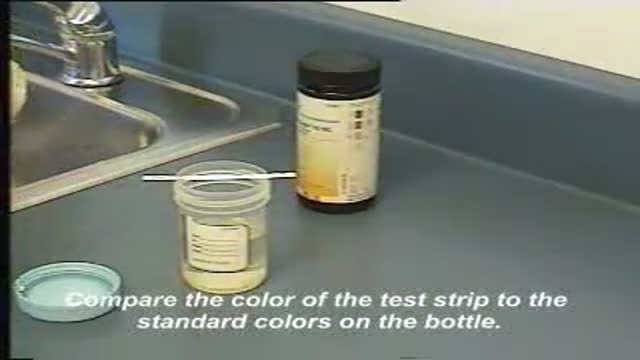
This video demonstrates how use a commercially-prepared "dip-stick" to test a random urine specimen for the presence of protein or glucose.

Upper gastrointestinal bleeding (sometimes upper GI, UGI bleed, Upper gastrointestinal hemorrhage, gastrorrhagia) refers to bleeding in the upper gastrointestinal tract, commonly defined as bleeding arising from the esophagus, stomach, or duodenum. In fact, the proportion of UGIB cases caused by peptic ulcer disease has declined, a phenomenon that is believed to be due to the use of proton pump inhibitors (PPIs) and H pylori therapy. Duodenal ulcers are more common than gastric ulcers, but the incidence of bleeding is identical for both.
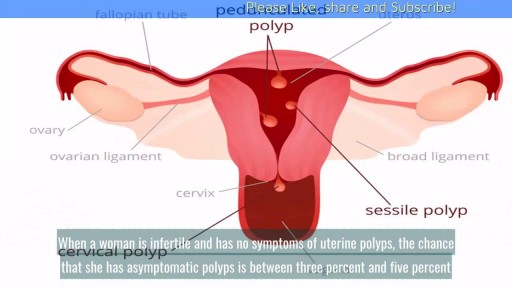
Uterine polyps, also called endometrial polyps, are usually small, bulb-shaped masses of endometrial tissue attached to the uterus by a stalk. They are soft, as opposed to uterine fibroids, which can grow much bigger and are made of hard muscle.

Colorectal surgeon Conor Delaney, MD, explains laparoscopic surgery for colon cancer, including how it works and what patients can typically expect before, during, and after the procedure.
Learn more about colon cancer at http://cancer.org/coloncancer

Ganglion Cyst Drainage

OB_A_1013
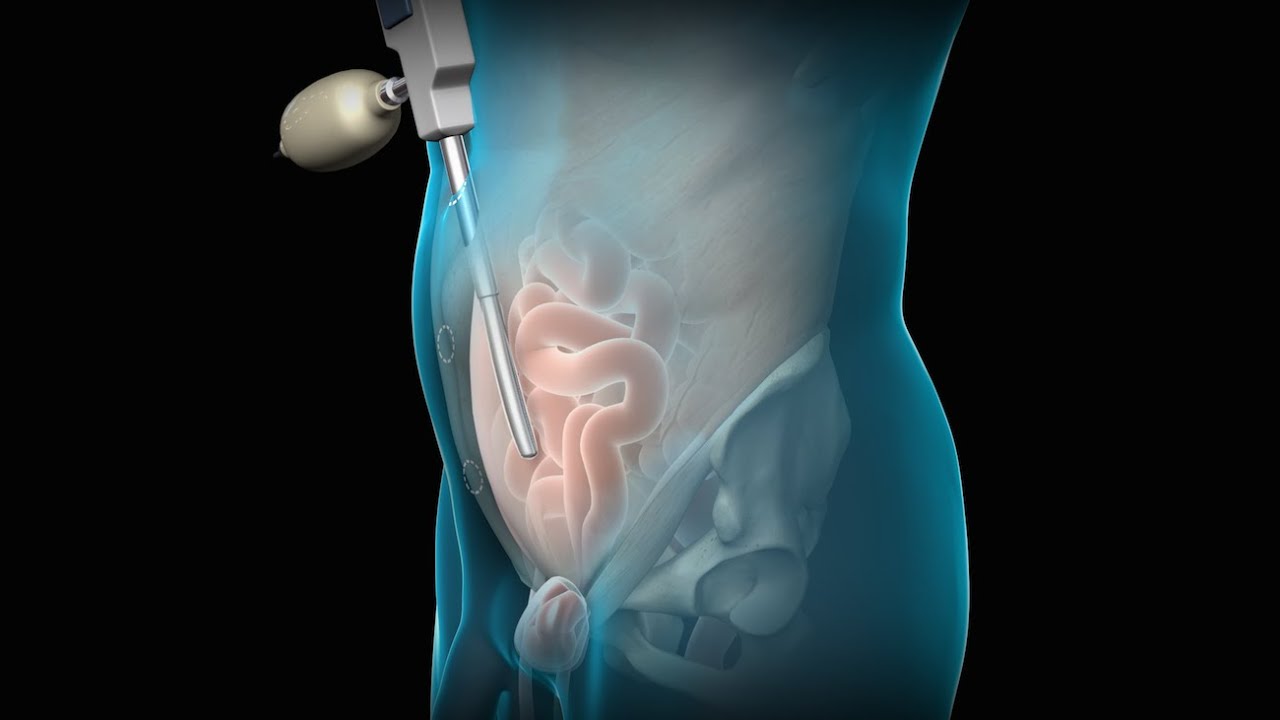
3D animation depicting the operating room and initial procedure preparing the patient for a laparoscopic hysterectomy. The patient is prepped and draped in the usual fashion and surrounded by the surgeon and surgical assistants. The skin is elevated, an infraumbilical incision is made, a trocar port is inserted through the incision and the abdomen is insufflated. Finally, a laparoscope is inserted into the port to allow for direct visualization of the uterus and the surgery can begin.
To view more animations and exhibits, visit our medical library: https://www.trialexhibitsinc.c....om/library/multimedi
Contact us on your next case for consulting, trial graphics, animations, medical illustrations or presentation services. 800-591-1123 [a]www.trialex.com[/a]
This video is for reference only. The video may not be otherwise used, reproduced nor modified. For more information to purchase a copy or permission to use this animation on your next case, project, website or TV, contact us at [a]www.trialex.com[/a] or 800-591-1123.
Copyright @ Trial Exhibits, Inc.
To license this video for patient education or content marketing, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=tephernia-030615
An inguinal hernia is a bulging of the intestine through a defect or weak spot in the wall of the lower abdomen. This video shows how inguinal hernias form and how they are treated.
#TotalExtraperitonealLaparoscopicInguinalHerniaRepair #TEP #laparoscopy
ANCE00200

Medication Through Running IV


What to expect during the day of a pediatric surgery at Sutter Children's Center Sacramento.

A Fistulotomy is the surgical opening or removal of a fistulous tract. They can be performed by excision of the tract and surrounding tissue, simple division of the tract, or gradual division and assisted drainage of the tract by means of a seton; a cord passed through the tract in a loop which is slowly tightened over a period of days or weeks.
Fistulas can occur in various areas of the human body, and the location of the fistula influences the necessity of the procedure. Some, such as ano-vaginal and perianal fistulas are chronic conditions, and will never heal without surgical intervention.

Adult Still's disease is a rare type of inflammatory arthritis that features fevers, rash and joint pain. Some people have just one episode of adult Still's disease. In other people, the condition persists or recurs. This inflammation can destroy affected joints, particularly the wrists. Treatment involves medications, such as prednisone, that help control inflammation

DMC Eye specialist restores a woman's vision by removing cataracts and installing an artificial lens. ~ Detroit Medical Center
