- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

enile implants are devices placed inside the penis to allow men with erectile dysfunction (ED) to get an erection. Penile implants are typically recommended after other treatments for ED fail. There are two main types of penile implants, semirigid and inflatable.

This video is showing the Femoral Nerve Block

Osteoarthritis
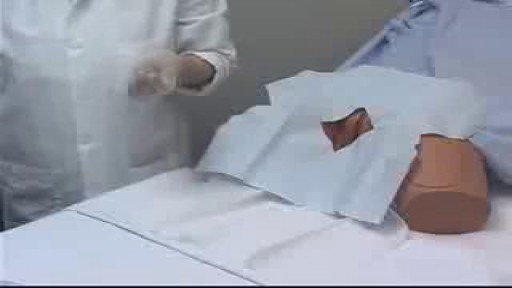
Female Catheter Insertion
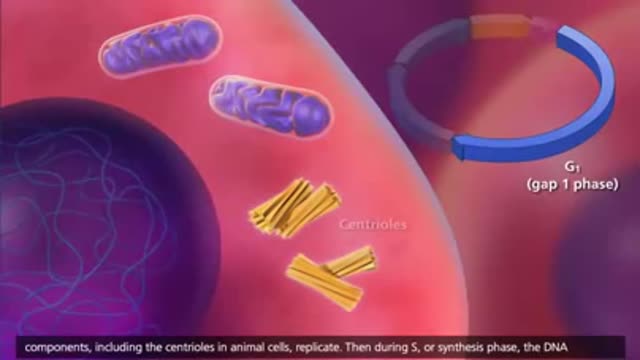
The cell cycle or cell-division cycle is the series of events that take place in a cell leading to its division and duplication of its DNA (DNA replication) to produce two daughter cells.
Symptoms of liver failure include vomiting, diarrhea and fatigue as well as the symptoms from stage 3. While the progression from cirrhosis to failure can take years, the damage is irreversible and leads to eventual death. The key to treating liver disease is to diagnose the condition as early as possible.
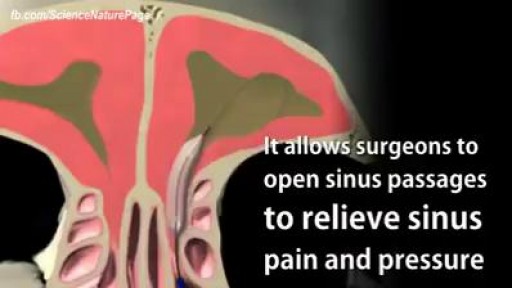
Balloon Sinuplasty for Sinus Infection
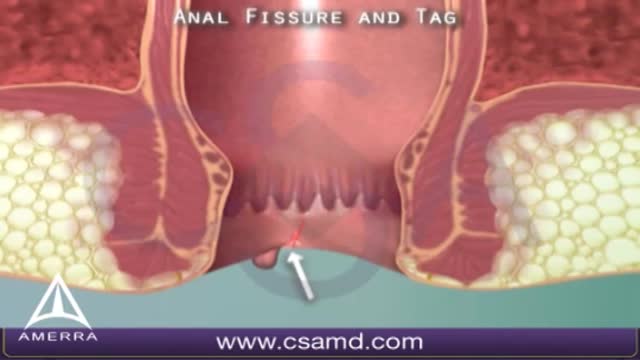
An anal fissure is a small tear in the thin, moist tissue (mucosa) that lines the anus. An anal fissure may occur when you pass hard or large stools during a bowel movement. Anal fissures typically cause pain and bleeding with bowel movements. You also may experience spasms in the ring of muscle at the end of your anus (anal sphincter). Anal fissures are very common in young infants but can affect people of any age. Most anal fissures get better with simple treatments, such as increased fiber intake or sitz baths. Some people with anal fissures may need medication or, occasionally, surgery.

Psychotic Depression Information

Delayed puberty is defined as the absence of any signs suggestive of puberty by 14 years of age. In this case, the patient's pubertal delay appears to be constitutional because of his positive family history, absence of syndromic features or systemic illness, and bone age of 12 years. Puberty correlates more closely with bone age than chronological age. On follow-up, the patient will most likely demonstrate a similar onset of puberty as his father.

Infected Hernia Mesh Repair Surgery Video

Most C-sections are done under regional anesthesia, which numbs only the lower part of your body — allowing you to remain awake during the procedure. A common choice is a spinal block, in which pain medication is injected directly into the sac surrounding your spinal cord

Watch this video to learn how and when to change a dressing for a child with a hemodialysis catheter. You should change your child's dressing if it becomes soiled with water or blood or if it comes off at home. Keeping a clean dressing on your child will limit risk of infection.

Otto Placik MD. a board certified Chicago based plastic surgeon presents Vulvar Vaginal Genital anatomy lesson reviewing the Vulva, Mons Pubis, clitoral hood, prepuce, frenulum, labia minora & majora, vagina, urethra and fourchette with surgical implications and techniques. Photos pictures and video of anatomic models are reviewed in detail on different models. Great for patients thinking about or planning before labiaplasty or vaginal cosmetic surgery

demonstrates how the Epley maneuver is performed to treat POSTERIOR canal BPPV affecting the right ear. Animation showing what is going on within the inner ear is also shown in the 2nd half of the video.

💪 Get our Knee Resilience program here: https://e3rehab.com/programs/r....esilience/knee-resil
In this video, I will walk you through a comprehensive rehab program for the most commonly injured knee ligament - the MCL.
💪 PROGRAMS: https://e3rehab.com/programs/
📩 MAILING LIST (exclusive deals, offers, and information): https://e3rehab.com/newsletter/
🏆 COACHING: https://e3rehab.com/coaching/
📝 ARTICLES: https://e3rehab.com/articles/
👕 APPAREL: https://e3rehab.com/clothing/
🎧 PODCAST: https://open.spotify.com/show/....5ZbaI145Bk94Guq7olMJ
AFFILIATES:
👟 Vivo Barefoot: Get 15% off all shoes! - https://www.vivobarefoot.com/e3rehab
📓 MASS (Monthly Research Review): http://bit.ly/E3MASS
📚 CSMi: https://humacnorm.com/e3rehab
🏋️ GYM EQUIPMENT: https://e3rehab.com/affiliates/
Follow Us:
YOUTUBE: https://www.youtube.com/@e3reh....ab?sub_confirmation=
INSTAGRAM: https://www.instagram.com/e3rehab
TWITTER: https://twitter.com/E3Rehab
FACEBOOK: https://www.facebook.com/e3rehab
TIKTOK: https://www.tiktok.com/@e3rehab
Intro (0:00)
Anatomy & Function (0:08)
Classification (1:11)
Treatment Options (1:46)
Bracing (3:30)
Rehab Overview (4:28)
Early Stage (5:27)
Mid-Stage(8:50)
Late Stage/Return to Sport (21:14)
Programming (22:13)
Summary (23:47)
---
Disclaimer: The information presented is not intended as medical advice or to be a substitute for medical counseling but intended for entertainment purposes only. If you are experiencing pain, please seek the appropriate healthcare professional.

To learn more about licensing this video for content marketing or patient education purposes, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=hiv-112513
This video, created by Nucleus Medical Media, shows the function of white blood cells in normal immunity. It also portrays how the human immunodeficiency virus (HIV) affects the immune system and causes acquired immunodeficiency syndrome (AIDS). Common types of antiretroviral medications used to treat HIV and AIDS are also shown.
#HIV #AIDS #HumanImmunodeficiencyVirus
ANH13111

DMC Interventional Radiologist Doctor Bruce Wolf uses minimally invasive surgery called Balloon Kyphoplasty to bring relief to a patient suffering from severe back pain caused by spinal compression fractures. This new procedure is especially beneficial to patients suffering from osteoporosis. ~ Detroit Medical Center

Excision of Rectovaginal Nodule

What is an ingrown hair cyst? An ingrown hair cyst refers to an ingrown hair that turns into a cyst — a large bump that extends between the skin’s surface and deep underneath it. The appearance is a cross between a regular ingrown hair and an acne cyst, though this is a different condition. These types of cysts are common among people who shave, wax, or use other methods to remove their hair. Although you may be eager to get rid of these cysts simply because of their appearance, it’s also important to watch for signs of an infection. Keep reading to learn what causes these cysts to form, plus how to treat them and prevent them from returning.
