- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

To get started, you need to find your pelvic floor muscles by stopping urination in midstream. If you succeed, you have located the right muscles. Once you have located your pelvic floor muscles, tighten the contraction for about 5 seconds, before relaxing for another 5 seconds.

Delayed puberty is defined as the absence of any signs suggestive of puberty by 14 years of age. In this case, the patient's pubertal delay appears to be constitutional because of his positive family history, absence of syndromic features or systemic illness, and bone age of 12 years. Puberty correlates more closely with bone age than chronological age. On follow-up, the patient will most likely demonstrate a similar onset of puberty as his father.
Emergency Physical Examination Lecture
Cardiology Physical Examination Lecture
Testicular Self Exam

In cases when the presentation is unclear, ultrasonography is the imaging methodology of choice. The characteristic finding is the presence of a "target sign". Ultrasonography is not required in patients with obvious clinical diagnosis (as seen in this patient). Such patients can proceed directly to treatment with diagnostic and therapeutic air (pneumatic) or water-soluble (hydrostatic contrast) enema.

Before Dr. Benjamin Carson became the first person to successfully separate twins conjoined at the head, before he had a TV movie made about his life, before he became known for his "gifted hands" and before he became head of pediatric neurosurgery at Johns Hopkins, Ben Carson was headed down the wrong path in life.
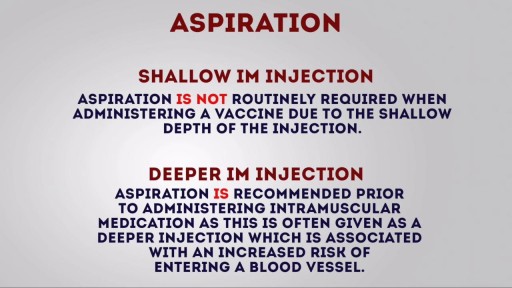
Intramuscular (IM) injection Tutorial for Nurses Video
ormal sperm densities range from 15 million to greater than 200 million sperm per milliliter of semen. You are considered to have a low sperm count if you have fewer than 15 million sperm per milliliter or less than 39 million sperm total per ejaculate.

In as many as 80% of cases, doctors don’t find the exact reason for a curved spine. Scoliosis without a known cause is what doctors call “idiopathic.” Some kinds of scoliosis do have clear causes. Doctors divide those curves into two types -- structural and nonstructural. In nonstructural scoliosis, the spine works normally, but looks curved. Why does this happen? There are a number of reasons, such as one leg’s being longer than the other, muscle spasms, and inflammations like appendicitis. When these problems are treated, this type of scoliosis often goes away.

New York surgeon Dr. Leo Keegan of 5th Ave. Millennium Surgery (http://www.5thavesurgery.com) speaks on the subject of liposuction.

A very funny song made by the staff of the Ob/Gyn Gangnam style
Cardiovascular surgery basically treats a number of diseases and medical disorders that affect your heart and the network of arteries and veins connecting it to every part of the body. https://goo.gl/iphEi9
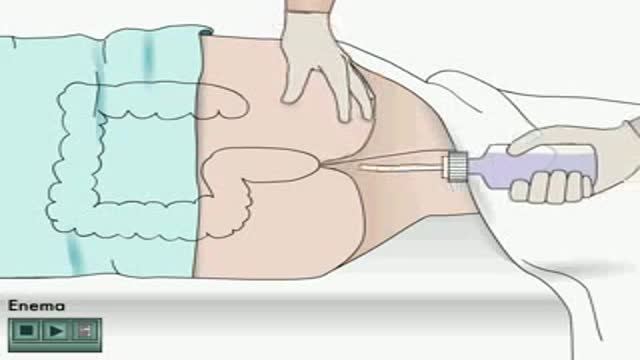
Enema how to apply Animation
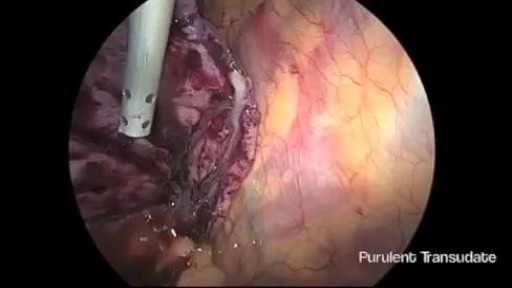
Thoracoscopic Management of Lung Abscess Before Empyema
Marfan syndrome is a disorder of connective tissue, the tissue that strengthens the body's structures. Disorders of connective tissue affect the skeletal system, cardiovascular system, eyes, and skin.

Intra-abdominal abscess continues to be an important and serious problem in surgical practice. Appropriate treatment is often delayed because of the obscure nature of many conditions resulting in abscess formation, which can make diagnosis and localization difficult. Associated pathophysiologic effects may become life threatening or lead to extended periods of morbidity with prolonged hospitalization. Delayed diagnosis and treatment can also lead to increased mortality; therefore, the economic impact of delaying treatment is significant.
Laparoscopic Colon Resection video

Cancer Patient Dances in OR before her Surgery
