- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A pneumothorax occurs when some of the tiny air sacs (alveoli) in a baby's lung become overinflated and burst. This causes air to leak into the space between the lung and chest wall (pleural space). The most common cause of pneumothorax is respiratory distress syndrome. This is a condition that occurs in babies who are born too early (premature). The baby's lungs lack the slippery substance (surfactant) that helps them stay open. Therefore, the tiny air sacs are not able to expand as easily. If the baby is put on a breathing machine (mechanical ventilator), there is extra pressure on the baby's lungs, which can sometimes burst the air sacs.

We will show how to know if you have a sports hernia. These are a few tests you can do on your own. Lower abdominal pain and tightness that increases with twisting and kicking. Stretching and exercises tend to make the discomfort increase.
Want more info? We have a free webinar that covers hip, groin, adductor, lower abdominal strains and sports hernia diagnosis in detail. Use this link to get access. https://bit.ly/37thtNF
#sportshernia #hernia #hippain
To work with us, contact us using this link https://bit.ly/3zCBnzZ or call us 714-502-4243. We have online programs, virtual and in-person options.
Costa Mesa, CA www.p2sportscare.com
Option 1: Groin On-Demand Webinar https://bit.ly/37thtNF
Option 2: Video Guide https://bit.ly/33aLIqC
Option 3 (the best): Work With Us https://www.p2sportscare.com/
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
Female Catheter Insertion

Purchase a license to download a non-watermarked copy of this video here: https://www.alilamedicalmedia.....com/-/galleries/all-
Voice by: Sue Stern.
©Alila Medical Media. All rights reserved.
Support us on Patreon and get FREE downloads and other great rewards: patreon.com/AlilaMedicalMedia
Perfect for patient education purposes.
All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition.
LASIK, or "laser-assisted in situ keratomileusis," is the most commonly performed laser eye surgery to treat myopia, hyperopia and astigmatism. The goal of the treatment is to reshape the cornea to correct the refractive error of the eye.
The cornea is the transparent dome-shaped structure in front of the eye. The cornea refracts light and accounts for about two-thirds of the eye's total optical power. Altering the curvature of the cornea changes the way light rays enter the eye. As a result, the light rays can be focused properly onto the retina for clearer vision.
For nearsighted people, the laser is used to flatten the cornea. For farsighted people, the cornea is made steeper. For patients with astigmatism, the laser is used to smooth the irregularly-shaped cornea into a more regular shape.
The outer layer of the cornea - the epithelium – is capable of replacing itself within a few days after being damaged or removed. The deeper layer of the cornea – the stroma, on the contrary, is a permanent corneal tissue with very limited regenerative capacity. The stroma, if reshaped by a laser, will remain that way permanently.
In this procedure, a thin, circular "FLAP" is created in the surface of the cornea to gain access to the permanent corneal tissue. This can be done with a mechanical cutting tool called a microkeratome, OR, for a blade-free experience, by a femtosecond laser. An excimer laser is then used to remove some corneal tissue to reshape the cornea. Excimer laser uses cool ultraviolet light beams to vaporize microscopic amounts of tissue in a precise manner to accurately reshape the cornea. The excimer laser is computer-controlled and is programmed based on the patient’s refractive error. The flap is then laid back in place and is allowed to heal.
LASIK eye surgery is mostly painless and can be completed within minutes. Improved vision can usually be seen overnight.
PRK, or photorefractive keratectomy, was the first type of laser eye surgery for vision correction and is the predecessor to the popular LASIK procedure. In PRK, NO flap is created. Rather, the epithelial cells on the eye surface are simply removed. An excimer laser is then used to reshape the cornea just like it does in LASIK.
The vision correction outcomes of PRK surgery are comparable to those of LASIK, but the recovery period is longer. This is because the epithelium is completely removed in PRK and it takes a few days to regenerate. PRK patients also have more discomfort and haziness of vision in the first few days after the surgery. Improved vision also takes longer to achieve.
PRK does, however, offer certain advantages. Because PRK does not involve creation of a flap, which contains both epithelial and deeper stromal tissue, the entire thickness of the stroma is available for treatment. The treatment range is therefore higher. This is particularly useful for patients with high levels of myopia or for those whose cornea is too thin for LASIK. PRK is also free of flap-related complication risks.
http://eliminar-seu-diabetes.good-info.co/ Tipos De Diabetes, Diabets, Alimentação Para Diabéticos, Diabetes Tipo Ii, Yacon Diabetes, https://youtu.be/iDK8jKuR_VQ É provável que se sinta identificado com alguma destas situações. Tem medo de uma complicação a longo prazo, como a perda da visão, a amputação dos dedos dos pés, de extremidades ou inclusive da morte? Quer terminar com as injeções diárias de insulina e as picadas nos dedos? Enfrenta diariamente o fato de que tem 80% de probabilidades de morrer com doenças cardíacas ou derrame cerebral? Sofre de excesso de peso que não pode eliminar, causada por seus medicamentos? Quer deixar de se sentir culpado por ter dietas especiais que complicam a organização da sua família? Está oprimido pelo cuidado e controle que diariamente esta doença precisa? Quer deixar de sofrer os terríveis efeitos secundários que provocam os medicamentos para o Diabetes? Sei o que se sente. pensar que não existe esperança, que não tem cura e que estamos condenados a viver doentes. Mas hoje Tenho Excelentes Notícias para lhe dar e posso garantir que o que você vai ler neste site será o mais importante que tenha lido em toda a sua vida.
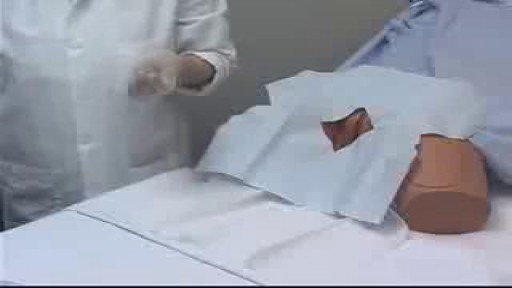
Intramuscular (IM) injection Tutorial for Nurses Video

McMurray's maneuver is used to detect the presence of meniscal tears. To detect a medial meniscal injury, the patient is put in a supine position with the knee in maximum flexion. One hand of the examiner is placed on the posteromedial margin of the involved knee and the other hand supports the foot. The tibia is then externally rotated, and the knee is extended slowly. The test is positive if there is an audible or palpable click or popping sensation during extension of the involved knee.

A patient who has a problem with proprioception can still maintain balance by using vestibular function and vision. In the Romberg test, the standing patient is asked to close his or her eyes. A loss of balance is interpreted as a positive Romberg's test.

Otto Placik MD. a board certified Chicago based plastic surgeon presents Vulvar Vaginal Genital anatomy lesson reviewing the Vulva, Mons Pubis, clitoral hood, prepuce, frenulum, labia minora & majora, vagina, urethra and fourchette with surgical implications and techniques. Photos pictures and video of anatomic models are reviewed in detail on different models. Great for patients thinking about or planning before labiaplasty or vaginal cosmetic surgery

A breech birth occurs when a baby is born bottom first instead of head first. Around 3-5% of pregnant women at term (37–40 weeks pregnant) will have a breech baby. Most babies in the breech position are born by a caesarean section because it is seen as safer than being born vaginally.

To avoid pregnancy and STDs, always remember to use a condom every time you have sex — including oral, vaginal, or anal sex. Whenever oral sex is being performed on a girl, a dental dam should be used. A guy receiving oral sex should wear a latex condom — or, if he or his partner is allergic to latex, a polyurethane condom.
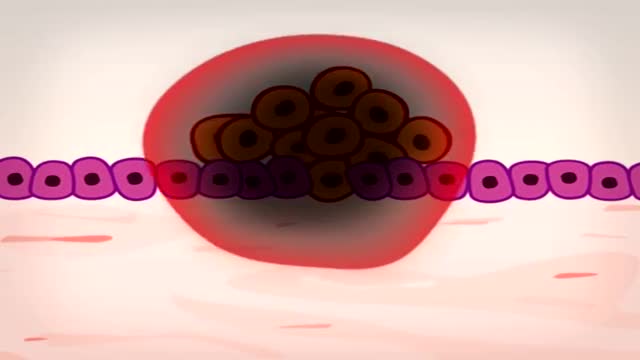
In 5 minutes find out how and why a normal cell becomes a cancer cell: risk factors and treatment.

The OrthoIllustrated® animation for total knee replacement is an educational tool to help patients better understand the diagnosis and treatment of arthritis.
- - - - -
Why Work Arthrex https://www.arthrex.com/job-seeker
Find an Arthrex Surgeon: https://doctorfinder.orthoillustrated.com
- - - - -
Join the Community:
LinkedIn: https://www.linkedin.com/company/arthrex
Facebook: https://www.facebook.com/Arthrex
Instagram: https://www.instagram.com/arthrex_inc/
Twitter: https://twitter.com/Arthrex
TikTok: https://www.tiktok.com/@arthrex
- - - - -
Arthrex Inc., headquartered in Naples, Florida, is a global leader in orthopedic surgical device design, research, manufacturing, and medical education. Arthrex develops and releases more than 1,000 new products and procedures every year to advance minimally invasive orthopedics worldwide.
For more information, visit https://www.arthrex.com
- - - - -
OrthoPedia is an innovative educational website that was created for anyone interested in learning about orthopedics from the first-year student to the experienced orthopedic surgeon.
Visit https://www.orthopedia.com to experience the future of Medical Education.
top 10 most incredible surgeries ever done

DMC Interventional Radiologist Doctor Bruce Wolf uses minimally invasive surgery called Balloon Kyphoplasty to bring relief to a patient suffering from severe back pain caused by spinal compression fractures. This new procedure is especially beneficial to patients suffering from osteoporosis. ~ Detroit Medical Center

High Quality Surgical videos and uncut stories ▶ https://surgeoncut.com

Toilet Training Boys, Training Potty, Best Way To Potty Train, What Age Do You Potty Train
http://potty-training-fast.good-info.co
Wanna have some fun imagining life without diapers?
Imagine if your child would disappear on their own
one minute and all of a sudden the next minute you
hear the toilet flush and the sink start to run.
Can you imagine it?
Life becomes so much easier the second your child
becomes potty trained and you start to wonder why
you didn't just get it over with sooner...
Would you start potty training right this weekend
if I handed you a guide that guaranteed to get your
child out of diapers in just 3 days?
Click the link below to check it out
http://potty-training-fast.good-info.co
Subscribe to our channel
http://potty-training-fast.blogspot.com/
https://www.youtube.com/watch?v=ck-4RTvP5F4
Toilet Training Boys, Training Potty, Best Way To Potty Train, What Age Do You Potty Train,
3day potty training,
toilet training tips for girls,
how to do potty training,
best potty training book,
potty training boys the easy way,
potty training activities,
how to potty training,
potty training video for toddlers,
when do you potty train,
how to potty train a kid,
potty training at 18 months,
havanese potty training,
how to potty train your baby,

Testosterone Booster, How To Get Testosterone, How To Improve Testosterone, Male Hormones
http://testosterone-booster.info-pro.co
Do This And Get Instantly Bigger Testicles
Today we're going to talk about the Stop And Go Method.
This tip is fun and easy to implement.
And your girl will absolutely love it Trust me on this
Here's the technique in a nutshell:
When doing the deed with your partner, take yourself just to the point of climax.
Then withdraw.
But don't just lay there while you wait for the peak to subside...
Kiss her, tease her, use your fingers, etc.
Watch this video and discover how to get much bigger testicles:
http://testosterone-booster.info-pro.co
Subscribe to our channel
http://natural-testosterone-boosters.blogspot.com/
https://www.youtube.com/watch?v=DPTeonpTBEM
Testosterone Booster, How To Get Testosterone, How To Improve Testosterone, Male Hormones,
how do you increase girth,
testosterone natural supplements,
improving sperm motility,
testosterone booster reviews,
girth increase,
how to increase my testosterone,
otc natural testosterone replacement,
testosterone increase,
are there foods that increase testosterone,
testosterona,
testosterone injections,
increasing testosterone naturally,
treatment for low testosterone,

Dr. James Wall performs a bilateral inguinial hernia repair surgical procedure.
Featured:
James Wall, MD
Assistant Professor of Surgery, Pediatric Surgery
Assistant Professor of Bioengineering (By Courtesy)
Lucile Salter Packard Children's Hospital
Micaela Esquivel, MD
Chief Resident of General Surgery

Use warm water and sea salt. Soak the wart for 10 to 15 minutes in warm salt water to moisten the skin. Scrape the dead skin layers off the wart using a nail file, pumice stone or mild sandpaper. You could also use your fingers, but wash them thoroughly before and after, as warts can easily spread.
