- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Posterior Chest Examination from the USMLE collection

It can treat spider veins and tiny varicose veins just under the skin's surface. ... (If you have poor blood circulation feeding these tiny veins, the larger "feeder" vein must first be treated with surgery, endovenous laser or radiofrequency treatment, or sclerotherapy.) Endovenous laser treatment.
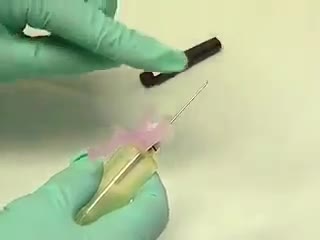
The venipuncture procedure is complex, requiring both knowledge and skill to perform. Each phlebotomist generally establishes a routine that is comfortable for her or him. Several essential steps are required for every successful collection procedure: Identify the patient. Assess the patient's physical disposition (i.e. diet, exercise, stress, basal state). Check the requisition form for requested tests, patient information, and any special requirements. Select a suitable site for venipuncture. Prepare the equipment, the patient and the puncture site. Perform the venipuncture. Collect the sample in the appropriate container. Recognize complications associated with the phlebotomy procedure. Assess the need for sample recollection and/or rejection. Label the collection tubes at the bedside or drawing area. Promptly send the specimens with the requisition to the laboratory.

Gallstone ileus is an important, though infrequent, cause of mechanical bowel obstruction, affecting older adult patients who often have other significant medical conditions. It is caused by impaction of a gallstone in the ileum after being passed through a biliary-enteric fistula. The diagnosis is often delayed since symptoms may be intermittent and investigations fail to identify the cause of the obstruction. The mainstay of treatment is removal of the obstructing stone after resuscitating the patient. Gallstone ileus continues to be associated with relatively high rates of morbidity and mortality.

Expressing the First Milk

http://www.bodysculptor.com. Dr. Otto Placik, Board Certified Chicago based plastic surgeon demonstrates the results of a muscle separation(rectus diastasis) repair using 3 dimesional CAT scan and photographic images

Juvenile polyposis syndrome (JPS) is a hereditary condition that is characterized by the presence of hamartomatous polyps in the digestive tract. Hamartomas are noncancerous (benign) masses of normal tissue that build up in the intestines or other places. These masses are called polyps if they develop inside a body structure, such as the intestines. The term “juvenile polyposis” refers to the type of polyp (juvenile polyp) that is found after examination of the polyp under a microscope, not the age at which people are diagnosed with JPS.

There are several types of hematomas and they are often described based on their location. Examples of hematomas include subdural, spinal, under the finger or toenail bed (subungual), ear, and liver (hepatic).


Watch that video to know How to Get Rid of Yellow Teeth Fast and Easy

Nystagmus is a vision condition in which the eyes make repetitive, uncontrolled movements. These movements often result in reduced vision and depth perception and can affect balance and coordination. These involuntary eye movements can occur from side to side, up and down, or in a circular pattern.
Testicle pain (testicular pain) is pain that occurs in or around one or both testicles. Sometimes testicle pain actually originates from somewhere else in the groin or abdomen, and is felt in one or both testicles (referred pain).

IMPLANT POCKETS - an educational animation explaining the different implant pockets


The IVF Lab
We are looking for 5 patients with knee pain who want to get significantly better in the next 30 days. Click this link to let me know you're interested and learn more.
https://www.drdavidgeier.com/work-with-me/contact/
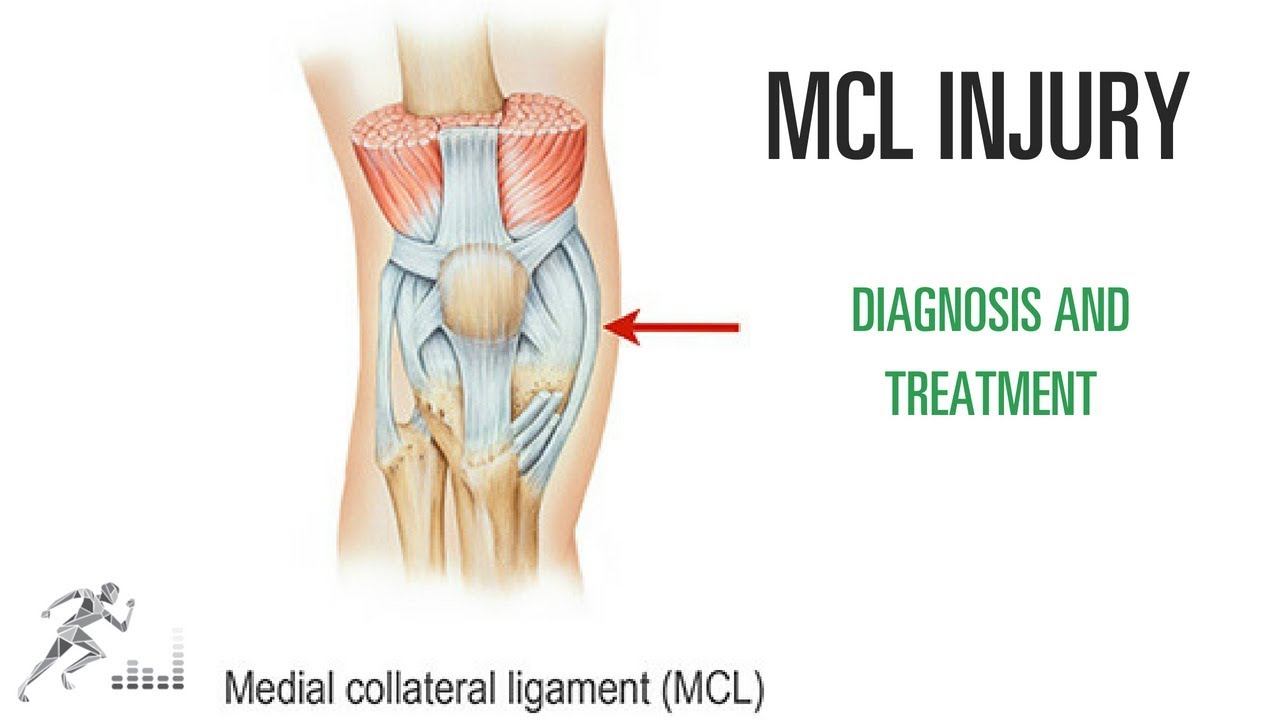
One of the most common knee injuries in contact and collision sports is a medial collateral ligament (MCL) injury. This is a ligament on the medial (side closest to the midline) side of your knee that provides stability against side-to-side stress to the knee. You might injure it by cutting maneuvers in sports like soccer or hockey. You can also suffer an MCL injury if another player hits you on the outside of your knee.
Please note: I don't respond to questions and requests for specific medical advice left in the comments to my videos. I receive too many to keep up (several hundred per week), and legally I can't offer specific medical advice to people who aren't my patients (see below). If you want to ask a question about a specific injury you have, leave it in the comments below, and I might answer it in an upcoming Ask Dr. Geier video. If you need more detailed information on your injury, go to my Resources page: https://www.drdavidgeier.com/resources/
The content of this YouTube Channel, https://www.youtube.com/user/drdavidgeier (“Channel”) is for INFORMATIONAL PURPOSES ONLY. The Channel may offer health, fitness, nutritional and other such information, but such information is intended for educational and informational purposes only. This content should not be used to self-diagnose or self-treat any health, medical, or physical condition. The content does not and is not intended to convey medical advice and does not constitute the practice of medicine. YOU SHOULD NOT RELY ON THIS INFORMATION AS A SUBSTITUTE FOR, NOR DOES IT REPLACE, PROFESSIONAL MEDICAL ADVICE, DIAGNOSIS, OR TREATMENT. You should consult with your healthcare professional before doing anything contained on this Channel. You agree that Dr. Geier is not responsible for any actions or inaction on your part based on the information that is presented on the Channel. Dr. David Geier Enterprises, LLC makes no representations about the accuracy or suitability of the content. USE OF THE CONTENT IS AT YOUR OWN RISK.
Unlike tears of the ACL, MCL injuries most often heal without surgery. You might need to wear a hinged knee brace for 2-6 weeks. The length of time you miss from sports or exercise varies depending on the location and severity of the injury.
In this video, I share my thoughts on the nature of an MCL injury, the diagnosis, the treatment options and return to sports.
Please remember, while I appreciate your questions, I cannot and will not offer specific medical advice by email, online, on my show, or in the comments at the end of these posts. My responses are meant to provide general medical information and education. Please consult your physician or health care provider for your specific medical concerns.

Watch that video to know The 8 Types Of Female Genital Discharge
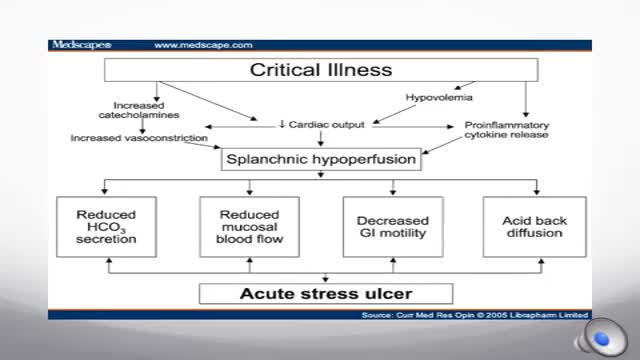
Stress-related mucosal disease (SRMD) is an acute, erosive gastritis representing conditions ranging from stress-related injury to stress ulcers (1, 2). Stress-related injury is superficial mucosal damage that presents primarily as erosions, whereas stress ulcers are deep, focal mucosal damage penetrating the submucosa with high risk for gastrointestinal bleeding (2, 3). Mucosal damage has been reported to occur during the first 24 hours of hospital admission in 75% to 100% of intensive care unit (ICU) patients (4, 5). Clinically important gastrointestinal bleeding can cause hemodynamic instability and increase the need for red blood cell transfusions (1). Significant bleeding may also increase the length of stay in the ICU and mortality (1).

UChicago Medicine organ transplant surgeon Dr. Rolf Barth explains a how the laparoscopic donor nephrectomy – also known as the single-port nephrectomy – procedure works to remove an organ donor’s kidney from their body to be transplanted into a recipient. This minimally invasive kidney donor transplant surgery allows living organ donors the get back to their lives more quickly than the traditional approach and leaves them with a nearly invisible scar in the belly button.
Learn more about living kidney donation: https://www.uchicagomedicine.o....rg/conditions-servic

**PLEASE READ FULLY
Purpose of the video is to help Esthetician’s review chapters in their text book to better prepare for State Bord testing, by simply reading and going over some of the material, it’s not intended to replace any teaching from any Beauty College. Every instructor does things different, Keep in mind I am in the state of Texas, also keep in mind that when in school students are to follow guidelines and might be required to do things a bit different, I teach my students the text book because that is where the state board questions come from and the goal is for them to pass their board exams. I also teach them and go over real working situations they might come across in the salon or spa.
* I am not affiliated with TDLR or PSI in any way
PSI Bulletin Link
https://candidate.psiexams.com/bulletin/display_bulletin.jsp?ro=yes&actionname=83&bulletinid=173&bulletinurl=.pdf
Glymed store: https://glymedplus.io/home/index?store=0011298
email: glamandbeyondinfo@gmail.com
