- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
As more couples explore anal sex, understanding the risks, rewards, and proper strategy is important. Here's what you need to know about safety and more.

Watch that Baby delivery Surgery video

The dilatation and Curettage procedure that is commonly performed (D and C)Part 2
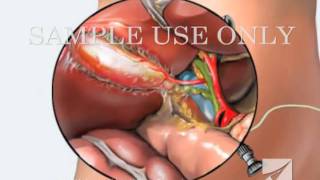
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026

Watch as Dr. Diaz performs a tummy tuck procedure on one of our patients!
A tummy tuck, also known as abdominoplasty, removes excess fat and skin and restores weakened muscles to create a smoother, firmer abdominal profile.
This patient as well wanted to receive liposuction in conjunction with the abdominoplasty. Liposuction sometimes referred to as "lipo" by patients, slims and reshapes specific areas of the body by removing excess fat deposits and improving your body contours and proportions.
The recovery time for a tummy tuck ranges anywhere from two to six weeks. The amount of recovery time you need depends on several factors of your surgery.
If you're interested in a consultation, contact us today! 424.235.6608

This video provides a demonstration of how to assess for transillumination when assessing scrotal swelling.
Read our step-by-step guide here: https://geekymedics.com/testic....ular-examination-osc
Check out our other awesome clinical skills resources, including:
• 🔥 Geeky Medics Bundles (discounted products): https://app.geekymedics.com/purchase/bundles/
• ✨ 1000+ OSCE Stations: https://app.geekymedics.com/pu....rchase/osce-stations
• 🏥 Geeky Medics OSCE Revision Book: https://app.geekymedics.com/purchase/book/
• 📝 150+ PDF OSCE Checklists: https://geekymedics.com/pdf-osce-checklists/
• 🗂️ 3000+ OSCE Flashcards: https://app.geekymedics.com/pu....rchase/flashcard-col
• 📱 Geeky Medics OSCE App: https://geekymedics.com/geeky-medics-app/
• 🩺 Medical Finals SBA Question Pack: https://app.geekymedics.com/pu....rchase/medical-stude
• 💊 PSA Question Pack: https://app.geekymedics.com/pu....rchase/prescribing-s
Subscribe to our newsletter to be the first to know about our latest content: https://geekymedics.com/newsletter/ ✉️
Join the Geeky Medics community: 👩👩👧👧
Twitter: http://www.twitter.com/geekymedics
Instagram: https://instagram.com/geekymedics
Facebook: http://www.facebook.com/geekymedics
Always adhere to your medical school/local hospital guidelines when performing examinations or clinical procedures. DO NOT perform any examination or procedure on patients based purely on the content of these videos. Geeky Medics accepts no liability for loss of any kind incurred as a result of reliance upon the information provided in this video.

► Get a free NCLEX NGN sample test today: http://lectur.io/nclexrnsampletestyt
► Create your free account today: http://lectur.io/nurseregisteryt
► If you’re an nursing educator or faculty member, visit: http://lectur.io/nursytb2u
In this video “How To Do An IM (Intramuscular) Injection” you will learn about:
►the steps in the administration of intramuscular medications
►the angle to position the syringe while administering an intramuscular injection
►the landmark to administer an intramuscular injection in the deltoid muscle
►5 tips for the safe administration of an intramuscular medication
►the steps of the Z-track method for intramuscular injections
►the role of aspirating blood during an intramuscular injection and evaluate whether this practice is currently in use
► This video is part of the Lecturio course “Fundamentals of Nursing: Clinical Skills”
► WATCH the complete course on http://lectur.io/njection
► THE PROF: Samantha Rhea MSN, RN has been a nurse since 2008 and a nursing faculty teacher since 2012. She has been recognized for clinical excellence as an interventional cardiology nurse and also led a Joint Commission Accredited Stroke Center. Ms. Rhea is an award-winning expert in clinical teaching and continues to maintain a current clinical practice and teaches at a University nursing program.
► LECTURIO is your smart tutor for nursing school: Learn the toughest NCLEX® topics with high-yield video lectures, integrated quiz questions, and more. Register now to study anytime and anywhere you want to: https://nursing.lecturio.com/#/
► CHECK OUT ALL NURSING COURSES:
Leadership Nursing: http://lectur.io/leadershipnursing
Dosage Calculation Nursing: http://lectur.io/dosagecalcnursing
Physiology Nursing: http://lectur.io/physiologynursing
Medical Surgical Nursing: http://lectur.io/medsurgnursing
Pharmacology Nursing: http://lectur.io/pharmacologynursing
NCLEX® Pharmacology Nursing: http://lectur.io/pharmnclexnursing
Pediatric Nursing: http://lectur.io/pediatricnursing
Study Skills Nursing: http://lectur.io/studyskillsnursing
Fundamentals of Nursing - Theory: http://lectur.io/fundamentalstheory
Fundamentals of Nursing - Clinical Skills: http://lectur.io/fundamentalsclinicalskills
Nursing Prerequisites: http://lectur.io/nursingprerequisites
Mental Health Nursing: http://lectur.io/mentalhealthnursing
Maternal-Newborn Nursing: http://lectur.io/maternalnewbornnursing
► INSTALL the free Lecturio app
iTunes Store: https://app.adjust.com/z21zrf
Play Store: https://app.adjust.com/b01fak
► SUBSCRIBE to our YouTube channel: http://lectur.io/subscribenursing
► WATCH MORE ON YOUTUBE: http://lectur.io/nursingplaylists
► LET’S CONNECT:
Facebook: www.facebook.com/lecturio.nursing
Instagram: www.instagram.com/lecturio_nursing
Join Discord Community: https://discord.gg/Ue95WDxCrp
TikTok: www.tiktok.com/@lecturio_nursing
LinkedIn: https://www.linkedin.com/company/lecturio-medical/
#nursingschool #nursingeducation #nursingclinicalskills #leadershipnursing #nclex #nursingfundamentals #nursingclinical #nursingskills

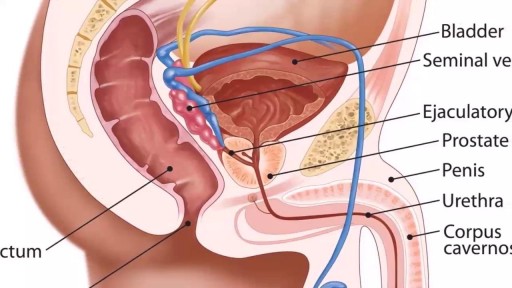
A testicular examination is mainly performed on male patients who present with testicular pathology e.g. pain, swelling, a lump. Although titled testicular examination it involves the examination of the penis, scrotum and testes. As this is an intimate examination it is pertinent to gain a good rapport with your patient, maintain good communication and ensure the patient’s dignity at all times. Remember to offer a chaperone for this skill. For the purposes of your exam, you will most likely be examining a mannequin.

Loyola Full Male Exam Part 3 A video from Loyola medical school, Chicago showing the full examination of the male

Dr. Jeffrey Ojemann, director of epilepsy surgery at Seattle Children's Hospital, explains a cutting-edge treatment for epilepsy: minimally invasive MRI-guided laser ablation surgery. Laser ablation surgery is much safer and more precise than other treatments, with fewer side effects.
A special thanks to patient Keoni Giauque.
For more information, visit: http://www.seattlechildrens.or....g/clinics-programs/n
"One Last Look" music rights via RoyaltyFreeMusic.com

Wow! Ultrasound guided internal jugular vein cannulation (long axis approach)

It is held in place with a balloon at the end, which is filled with sterile water to prevent the catheter from being removed from the bladder. The urine drains through the catheter tube into a bag, which is emptied when full. The procedure to insert a catheter is called catheterization.

Surgical cutting and removal of a deep skin cyst Medical Videos
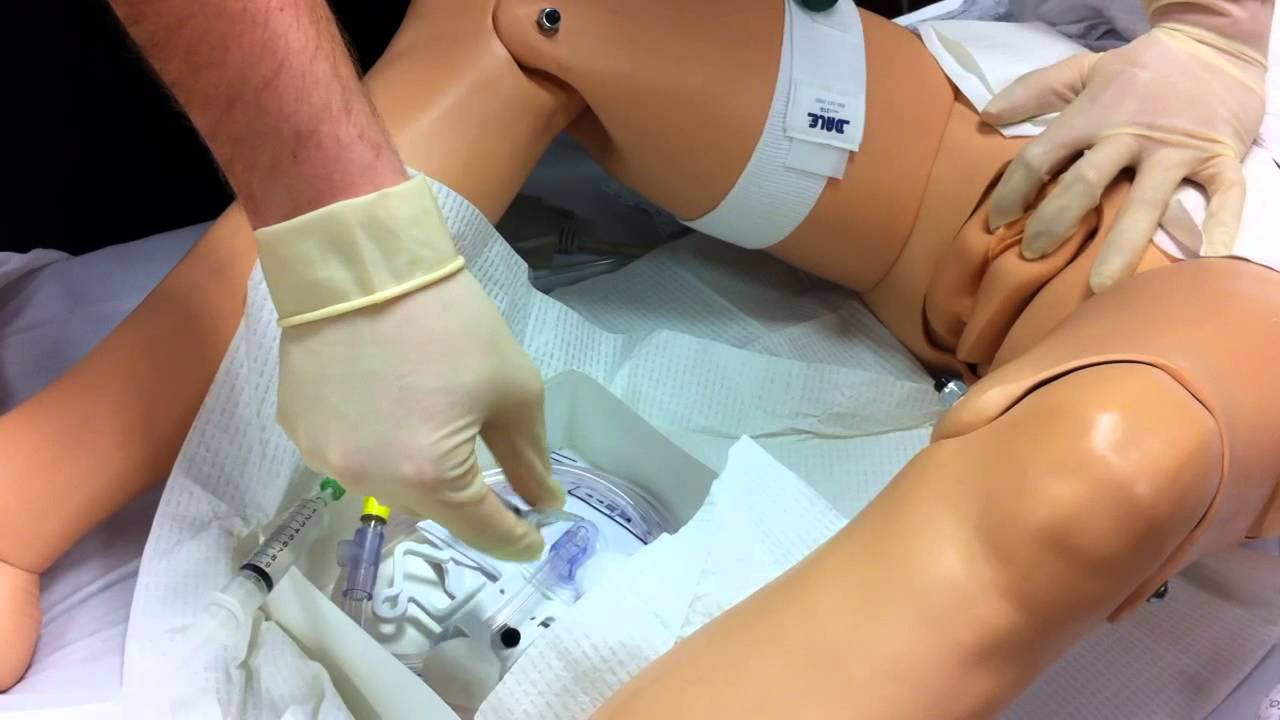
Watch that Female Foley Genital Catheter Insertion Procedure

This is how Paraumbilical hernia looks like and how it is examined although it looks very simple but in exam it can be very difficult to perform all steps in small amount of time. This can be short case or even long of #cpsp #fcps #mbbs #medicalstudent #mbbsexams #plab2 #plab #plab1 and MS #genernalknowledge #surgery exams
#para-umbilical hernia
#umbilical hernia #paraumbilical #hernia repair#laparoscopic paraumbilical hernia repair. #umbilical defect, #vetral hernia surgery. #herniatreatment #herniatreatment #ventral hernia hernia,#laparoscopic ventral hernia repair,umbilicus,carl lowe jr,hernia repair,training,north carolina,hernia repair surgery,charlotte,operation,laparoscopic,bulge,surgery,surgeon,dr. lowe,ipom repair,live surgery,mesh,
#mesh #ipom repair

Watch that Baby Abortion Medical Procedure

This patient presented to the ER for umbilical pain and had a history of umbilical hernia. He was concerned about the possibility of incarceration of the hernia.
In this video we explain how the clinical exam helps to differentiate a simple painful hernia from an incarcerated one.
***Thanks to the patient for sharing his history and exam with YouTube world***

Watch that Full Human Body Medical Anatomy Autopsy
Pelvic examinations during labor are used for several purposes, among them assessment of cervical dilatation, effacement, station of the presenting part, presentation, position, and pelvic capacity.Instruction in these techniques is particularly important for those health care providers involved in labor management, including physicians, nurses, midwives, paramedics and EMT personnel.

Alexandra J. Golby, MD, Director, Image-guided Neurosurgery at Brigham and Women’s Hospital, discusses technological advancements to improve the precision of surgery to remove brain tumors.
It’s estimated that each year nearly 80,000 people are diagnosed with primary brain tumors and 100,000 with metastatic brain tumors. Nearly everybody is at risk for developing a brain tumor. Brain tumors can affect people from childhood to the last years of their lives. Men are slightly more affected than women and the causes of most brain tumors are not known.
There are a number of unique challenges in treating brain tumors. One challenge is that primary tumors can have indistinct margins that are difficult to see. Another challenge is that the tissue around a brain tumor is uniquely important and may impact things like language, visual and motor function.
The AMIGO Suite, opened in 2011 at Brigham and Women’s Hospital, is the Advanced Multimodality Image Guided Operating Suite. It's an NIH-funded national center which was developed with the goal of translating technological advances into improvements in surgical and interventional care for patients. In the AMIGO Suite, there is an intraoperative MRI scanner which can be brought in and out of the operating room during surgery to help surgeons visualize a patient’s tumor better.
Image-guided surgery uses the information obtained from advanced imaging and translates that into the planning and execution of surgery by acquiring high resolution and specialty structural images of the brain and also functional images of the brain. These images can be registered to one another and then to the patient's head during surgery. This allows surgeons to pinpoint the location of the tumor as well as the areas that we would like to preserve, areas that serve critical brain functions are located.
One of the big challenges, even with image-guided surgery, is that as we perform the surgery, the configuration of the brain is changing, and we call that brain shift. And it's due to changes in the brain itself and also as we remove tissue, things are constantly shifting and moving. When we're talking about doing brain tumor surgery, a few millimeters of movement can be a big difference. How to measure and track brain shift is an important area of research and a number of technologies are being studied to understand how to measure brain shift during surgery.
The development of various intraoperative imaging technologies allows surgeons to provide the most accurate surgical treatment for each individual patient.
Learn more about precision brain surgery at Brigham and Women’s Hospital:
https://www.brighamandwomens.o....rg/neurosurgery/brai
