- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
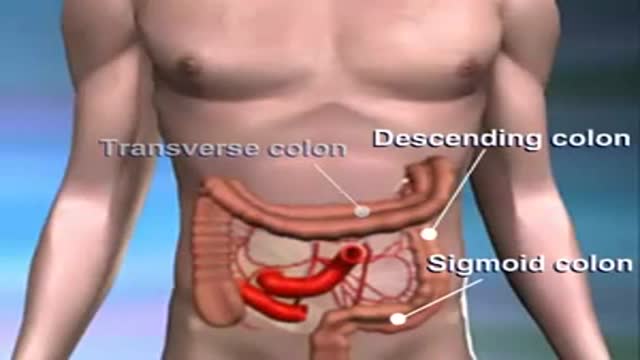
Colon cancer usually begins as a non-cancerous growth. If caught early enough, it can be safely removed with little to no complications.

The products of a surgical abortion.

http://drraewynteirney.com.au/video/
http://drraewynteirney.com.au/....about-dr-raewyn-teir
Dr Raewyn Teirney - fertility specialist and Gynaecologist in Sydney shows a video recording of a laparoscopy for a woman with infertility and pelvic pain.

CORRECTION: After review of this video, it is clear that this video is of a baby who is near full term (40 weeks) based on the size. Late trimester "abortions" are defined only to viability of a baby (24 weeks) A 24 week baby is much smaller than this baby shown and by definition this is not a late "abortion" procedure. The proper labeling of this video should be management of a deceased breech baby with "head entrapment" as this was almost certainly a naturally occuring delivery and an OB nightmare (Reviewed by Dr. Frederick Bright)

Observation of both jugular veins can provide a reliable indication of the volume and pressure in the right side of the heart since internal jugular veins pulsate in response to phasic changes in right atrial pressure. Proper positioning of the patient to increase the effects of gravity enhances distention of the jugular veins and, therefore, increases the ability to observe venous pulsations.
ADH's job is to act on the kidneys to promote water reabsorption. In this lesson, we'll compare and contrast diabetes insipidus, or DI, in which there is too little ADH, and syndrome of inappropriate antidiuretic hormone secretion , or SIADH, in which there is too much ADH.

A stepwise approach to the causes and diagnosis of Anaemia in clinical practice. This presentation includes the all important concept of the Reticulocyte production index. Discussion of Hereditary and acquired causes of Anaemia has been included in detail.

This video shows how to insert a catheter in a baby girl
An old video showing how to give an enema
The mainstay of treatment is usually medication, talk therapy, or a combination of the two. Increasingly, research suggests these treatments may normalize brain changes associated with depression.

A video showing the surgery of vaginal hysterectomy Operation
Prostate Health and Cancer Seminar features nationally renowned physicians and scientists presenting the most current study and practices for the diagnosis and treatment of prostate cancer. This day-long program offers in-depth exploration of prostate issues that range from monitoring PSA counts to cutting-edge research to current treatment trends.

Watch that video of Huge 132 lbs Testicles Tumor Removal Surgery
http://tinnitus-solution.info-pro.co --- Ear Infection, Loud Ringing In Ears, Tinnitus Suicide, Ear Is Ringing, Tinnitus One Ear, Tinnitus. Do you suddenly get up in the middle of the night hearing strange noises? Yes it can definitely be frightening, more so when you cannot find the source. Now consider for a moment that these sounds are coming from within you. Most people would be stunned to know that. Many of us do not even know that our internal organs can make sounds. Let us try to see whether you actually heard these noises or not, and if you did, where did they come from. Now before anything, let us get this straight - yes, you actually heard those noises. No, they are not a result of a creative mind that imagined things in slumber. But having said that, it is also true that there is indeed no source of the sounds you heard. So what is it? Confused? This is a classic case of tinnitus. What is tinnitus? What you experienced last night (or did you just get up from sleep and switch on the computer) is a classic case of tinnitus. This is a medical condition wherein a person hears all kinds of strange clicking, ringing, buzzing, whistling or hissing sounds within the ear. What's so worrisome about this condition for a lot of people is that, there's actually no physical source of these sounds. What makes it even worse is that, no one else seems to hear them. Frankly, these people cannot be really blamed. Naturally, if you cannot see where the sound is coming from, and if you keep hearing it, you are bound to get worried. In tinnitus, the sounds a person hears are actually perceptions. Since there's no actual source, they are often referred to as "phantom noises". Will it help you if you knew that about 8% of all people in the US suffer from tinnitus? Perhaps not, but at least now you know that you are not alone who hears these strange noises. Cure tinnitus. this simple, but effective system to erasing Tinnitus out of your life for good has now helped cure over 105,302 people of all the frustrating ringing, hissing, buzzing. Even if you’ve tried every single tinnitus treatment or remedy under the sun. 100% natural tinnitus cure click here: http://tinnitus-solution.info-pro.co
http://www.vaginal-ultrasound.com A demonstration of a vaginal ultrasound.

Watch as Dr. Diaz performs a tummy tuck procedure on one of our patients!
A tummy tuck, also known as abdominoplasty, removes excess fat and skin and restores weakened muscles to create a smoother, firmer abdominal profile.
This patient as well wanted to receive liposuction in conjunction with the abdominoplasty. Liposuction sometimes referred to as "lipo" by patients, slims and reshapes specific areas of the body by removing excess fat deposits and improving your body contours and proportions.
The recovery time for a tummy tuck ranges anywhere from two to six weeks. The amount of recovery time you need depends on several factors of your surgery.
If you're interested in a consultation, contact us today! 424.235.6608

Your kids are going to love brushing! Follow these tips and find out how brushing your teeth can be fun and effective for the whole family.

SINUS LIFT SURGERY surgical procedure which aims to increase the amount of bone in the posterior maxilla (upper jaw bone), in the area of the premolar and molar teeth, by lifting the lower Schneiderian membrane (sinus membrane) and placing a bone graft.

aasd

Professional breast exam
