- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A video showing breast examination after breast implants
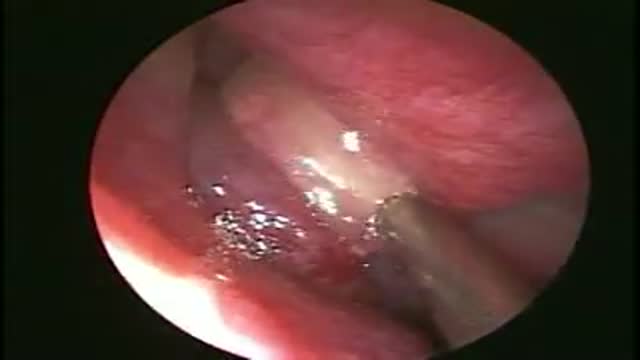
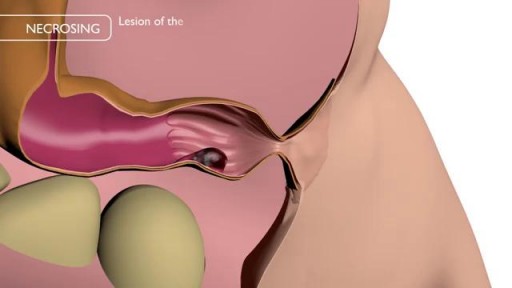
Drainage of a maxillary Sinus pyocoele
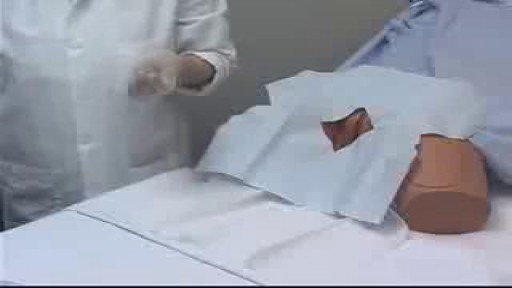
Female Catheter Insertion

Detailed examination of the joints is usually not included in the routine medical examination. However, joint related complaints are rather common, and understanding anatomy and physiology of both normal function and pathologic conditions is critically important when evaluating the symptomatic patient. By gaining an appreciation for the basic structures and functioning of the joint, you'll be able to "logic" your way thru the exam, even if you can't remember the eponym attached to each specific test!
Though the risk of HIV transmission through oral sex is very low, but several factors might increase the risk, including sores in the mouth or vagina or on the penis, bleeding gums, having an oral contact with menstrual blood, and the presence of other sexually transmitted diseases. But still the risk is low. by the way better to think twice before having the Oralsex with strangers. because you are not safe 100%.

Removal of Infected Hernia Mesh

New Minimally Invasive Procedure with No Pain or Downtime… From Dr. Michael Goodman, Caring For Women Wellness Center Laser Vaginal Tightening for Improved Sexual Pleasure and Relief from Minimal Urinary Incontinence Laser Vaginal Therapy for reversing Vaginal Atrophy (Good also for Breast Cancer Survivors with Vaginal Atrophy)
New Hemorrhoids Treatment Method

new study about the size of penis

Worst Nail Infection: Paronychia

Worms Inside Human Stomach

Watch this video to learn how and when to change a dressing for a child with a hemodialysis catheter. You should change your child's dressing if it becomes soiled with water or blood or if it comes off at home. Keeping a clean dressing on your child will limit risk of infection.

Otto Placik MD. a board certified Chicago based plastic surgeon presents Vulvar Vaginal Genital anatomy lesson reviewing the Vulva, Mons Pubis, clitoral hood, prepuce, frenulum, labia minora & majora, vagina, urethra and fourchette with surgical implications and techniques. Photos pictures and video of anatomic models are reviewed in detail on different models. Great for patients thinking about or planning before labiaplasty or vaginal cosmetic surgery
Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia. Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.

Understanding the process of getting braces

This video: Blisters caused by friction or minor burns do not require a doctor's care. New skin will form underneath the affected area and the fluid is simply absorbed. Do not puncture a blister unless it is large, painful, or likely to be further irritated. The fluid-filled blister keeps the underlying skin clean, which prevents infection and promotes healing.

SUBSCRIBE: https://www.youtube.com/c/TVNe....phrologist?sub_confi
An animation of blood flow inside the Hemodialysis circuit.
About Dr. Rifai:
Dr. Ahmad Oussama Rifai is certified by the American Board of Internal Medicine (ABIM) in the specialty of Internal Medicine and the sub-specialty of Nephrology.
MEET DR. RIFAI
https://www.thevirtualnephrologist.com/rifai/
Follow The Virtual Nephrologist on SOCIAL MEDIA:
-Facebook: https://www.facebook.com/thevirtualnephrologist
-Instagram: https://www.instagram.com/thevirtualnephrologist/
-Twitter: https://twitter.com/VNephrologist
Schedule a virtual consult:
https://www.thevirtualnephrolo....gist.com/schedule-a-
Best wishes for great health | The Virtual Nephrologist

DMC Interventional Radiologist Doctor Bruce Wolf uses minimally invasive surgery called Balloon Kyphoplasty to bring relief to a patient suffering from severe back pain caused by spinal compression fractures. This new procedure is especially beneficial to patients suffering from osteoporosis. ~ Detroit Medical Center
http://eliminar-seu-diabetes.good-info.co/ Tipos De Diabetes, Diabets, Alimentação Para Diabéticos, Diabetes Tipo Ii, Yacon Diabetes, https://youtu.be/iDK8jKuR_VQ É provável que se sinta identificado com alguma destas situações. Tem medo de uma complicação a longo prazo, como a perda da visão, a amputação dos dedos dos pés, de extremidades ou inclusive da morte? Quer terminar com as injeções diárias de insulina e as picadas nos dedos? Enfrenta diariamente o fato de que tem 80% de probabilidades de morrer com doenças cardíacas ou derrame cerebral? Sofre de excesso de peso que não pode eliminar, causada por seus medicamentos? Quer deixar de se sentir culpado por ter dietas especiais que complicam a organização da sua família? Está oprimido pelo cuidado e controle que diariamente esta doença precisa? Quer deixar de sofrer os terríveis efeitos secundários que provocam os medicamentos para o Diabetes? Sei o que se sente. pensar que não existe esperança, que não tem cura e que estamos condenados a viver doentes. Mas hoje Tenho Excelentes Notícias para lhe dar e posso garantir que o que você vai ler neste site será o mais importante que tenha lido em toda a sua vida.
