- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
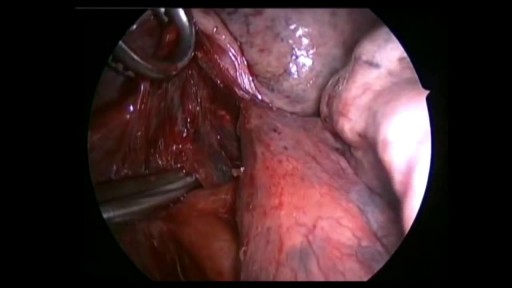
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Arterial line placement is a common procedure in various critical care settings. Intra-arterial blood pressure (BP) measurement is more accurate than measurement of BP by noninvasive means, especially in the critically ill. [1] Intra-arterial BP management permits the rapid recognition of BP changes that is vital for patients on continuous infusions of vasoactive drugs. Arterial cannulation also allows repeated arterial blood gas samples to be drawn without injury to the patient.
If you have a lung disease, a type of surgery called a lobectomy is one treatment option your doctor may suggest. Your lungs are made up of five sections called lobes. You have three in your right lung and two in your left. A lobectomy removes one of these lobes. After the surgery, your healthy tissue makes up for the missing section, so your lungs should work as well or better than they did before.
symptoms of kidney dysfunction. I find kidney dysfunction in my patients very frequently. Lower back pain is a common indicator that the kidneys are starting to become irritated. Yes, lower back pain can come from many different areas, but one of the areas I always rule out is kidney congestion.

Hemorrhoidectomy

Watch that video to see How Snake Poison Coagulates Human Blood

Elizabeth Stephens, MD joined the Department of Cardiovascular Surgery at Mayo Clinic Rochester, Minnesota in 2019. To learn more about Dr. Stephens’ practice: https://www.mayoclinic.org/bio....graphies/stephens-el
Elizabeth H. Stephens, M.D., Ph.D., is an Assistant Professor of Surgery in Cardiovascular Surgery specializing in congenital cardiac surgery. She received her medical degree from Baylor College of Medicine and Ph.D in Bioengineering from Rice University focusing on tissue engineering heart valves. Her adult cardiothoracic training was completed at Columbia University and congenital training at Lurie Children's Hospital in Chicago. Her clinical areas of expertise include the treatment of:
• Neonates, infants, and children with complex congenital heart disease
• Adult patients with congenital heart disease, including patients previously repaired
• Valve disease, including Ebstein's anomaly
• Pediatric patients with heart failure, including mechanical circulatory support and heart transplantation
• Patients with vascular rings and tracheal stenosis
In addition to her clinical areas of expertise, Dr. Stephens is active in outcomes research relative to congenital heart disease and is extensively published on various cardiac surgery conditions. She has a particular interest in education, including serving on national committees and mentoring trainees of all levels.
http://permanently-cure-your-ulcer.info-pro.co/ Symptoms Of An Ulcer, H Pylori Natural Treatment, H Pylori Treatment Natural, Diet For H Pylori. Are You Sure You Have An Ulcer? There are many symptoms that are associated with ulcers. Some ulcer sufferers only experience mild symptoms while others experience more severe. The more common symptoms of an ulcer are listed below. Abdominal discomfort is the most common symptom of an ulcer. This discomfort usually: is a dull, gnawing ache. • comes and goes for several days or weeks. • occurs 2 to 3 hours after a meal. • occurs in the middle of the night (when the stomach is empty). • is relieved by eating. • is relieved by antacid medications. Other symptoms include: • weight loss • poor appetite • bloating • burping • nausea • vomiting If you have some or all of these symptoms, it’s a good indicator that you may have an ulcer or be developing an ulcer. Discover my 100% natural cure for ulcers. click here. http://permanently-cure-your-ulcer.info-pro.co/

Rapid cycling is a pattern of frequent, distinct episodes in bipolar disorder. In rapid cycling, a person with the disorder experiences four or more episodes of mania or depression in one year

A doctor pops a giant cyst on a boy's eye and films the whole thing. As the big cyst pops, puss oozes out.

A 29 years old man lost his left wrist in car turn over in 2014. this video is taken 1 year after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic

MotionLit can help you multiply the value of your case by portraying the mechanisms of injuries in a 3D Accident Reconstruction Animation. Call (855)850-0650 or visit motionlit.com to learn & earn more for your client!
MotionLit is a one-stop-shop for litigators, offering complete trial services from video production, animation, litigation support, exhibit design, trial technician, and video depositions. Our visuals have proven to help attorneys obtain record-breaking verdicts with our persuasive trial presentations, settlement documentaries, and demonstratives.
Contact Us At:
www.motionlit.com
(213) 291 9141
info@motionlit.com
Follow Us On:
Twitter: @motionlit
Instagram: https://www.instagram.com/motionlit/
Facebook: https://www.facebook.com/MotionLit/

This animated video reviews cochlear implants, used for people with profound hearing loss.

Successful External Cephalic Version (ECV) - Turning a breech baby in less than 30 seconds!

Head Eye and ENT Physical Examination
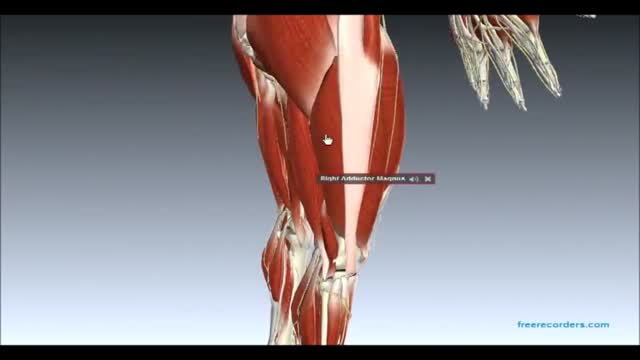
Muscles and Nerves of Lower Limb

Alcoholic hepatitis is inflammation of the liver caused by drinking alcohol. Alcoholic hepatitis is most likely to occur in people who drink heavily over many years. However, the relationship between drinking and alcoholic hepatitis is complex. Not all heavy drinkers develop alcoholic hepatitis, and the disease can occur in people who drink only moderately. If you're diagnosed with alcoholic hepatitis, you must stop drinking alcohol. People who continue to drink alcohol face a high risk of serious liver damage and death.

Tracheostomy

Recovery Tips
LASIK eye surgery is the best known and most commonly performed laser refractive surgery to correct vision problems. The total recovery time is 1 to 2 weeks. However, vision may fluctuate slightly over the next 2 months.
Avoid watching television or reading for the first few days.
You can get back to work after 1 week.
Avoid applying pressure on the eyes for 7 days.
Avoid dust, smoke, yard and garden work, and eye make-up.
Wear eye shields at night given by a surgeon for 1 week.
Driving is allowed after 4 to 5 days.
Avoid swimming or using a hot tub for 2 weeks after surgery.
While using the computer, take frequent breaks and lubricate your eyes with artificial tears.
For treatment assistance in your country or abroad:
Email: hello@vaidam.com
Phone/WhatsApp/Viber: +91-9650001746
Website: www.vaidam.com
Vaidam is an ISO and NABH accredited medical assistance company. Patients from 100+ countries have used our services.
Useful Links:
India
Doctors: https://www.vaidam.com/doctors/opthalmology/lasik-procedure/india
Hospitals: https://www.vaidam.com/hospitals/opthalmology/lasik-procedure/india
Cost of Lasik Eye Surgery: https://www.vaidam.com/cost/lasik-procedure-cost-in-india
Turkey
Doctors: https://www.vaidam.com/doctors/opthalmology/lasik-procedure/turkey
Hospitals: https://www.vaidam.com/hospitals/opthalmology/lasik-procedure/turkey
Laparotomy Closure Abdomen Animation

Sean Langenfeld, M.D., UNMC College of Medicine
