- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
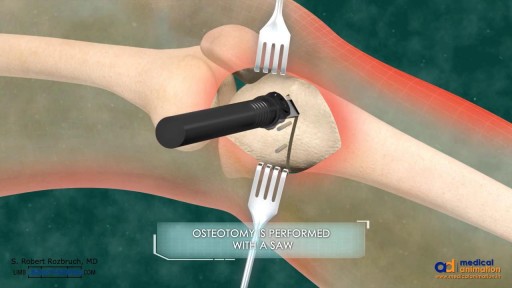
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
MRI scan of a 23-week-pregnancy
Pulmonary hypertension is a type of high blood pressure that affects the arteries in your lungs and the right side of your heart. In one form of pulmonary hypertension, tiny arteries in your lungs, called pulmonary arterioles, and capillaries become narrowed, blocked or destroyed. This makes it harder for blood to flow through your lungs, and raises pressure within your lungs' arteries. As the pressure builds, your heart's lower right chamber (right ventricle) must work harder to pump blood through your lungs, eventually causing your heart muscle to weaken and fail. Some forms of pulmonary hypertension are serious conditions that become progressively worse and are sometimes fatal. Although some forms of pulmonary hypertension aren't curable, treatment can help lessen symptoms and improve your quality of life. Pulmonary hypertension care at Mayo Clinic
Pediatric measurements: length, body weight...etc.
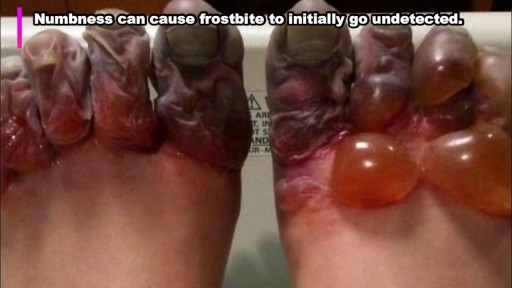
rostbite refers to the freezing of body tissue (usually skin) that results when the blood vessels contract, reducing blood flow and oxygen to the affected body parts. Normal sensation is lost, and color changes also occur in these tissues.

Sclerotherapy for varicose veins

Breech Baby Position Exercise!

The Spirotome belongs to the Direct & Frontal type of biopsy systems for taking large core biopsy from virtually every soft tissue in the body. The FDA has approved 13 applications. This video shows how easy it is to take a large core from a thoracic wall tumor mass. The size and quality of the sample allows quantitative molecular biology.

Benefits of Breast Feeding

Premature ejaculation occurs when a man ejaculates sooner during sexual intercourse than he or his partner would like. Premature ejaculation is a common sexual complaint. Estimates vary, but as many as 1 out of 3 men say they experience this problem at some time. As long as it happens infrequently, it's not cause for concern. However, you may meet the diagnostic criteria for premature ejaculation if you: Always or nearly always ejaculate within one minute of penetration Are unable to delay ejaculation during intercourse all or nearly all of the time Feel distressed and frustrated, and tend to avoid sexual intimacy as a result Both psychological and biological factors can play a role in premature ejaculation. Although many men feel embarrassed to talk about it, premature ejaculation is a common and treatable condition. Medications, counseling and sexual techniques that delay ejaculation — or a combination of these — can help improve sex for you and your partner.

This video will cover, in detail, the motor, sensory, reflect components of a neurological examination.
This video is created for the UBC Medicine Neurology Clinical Skills curriculum as part of MEDD 419 FLEX projects.
Filmed, written, and directed by:
John Liu
Vincent Soh
Chris Calvin
Kashi (Siyoung) Lee
Kero (Yue) Yuen
Ge Shi
Doctor - Dr. Jason Valerio (Department of Neurology, UBC)
Supervised by:
Dr. Alex Henri-Bhargava (Department of Neurology, UBC)
Zac Rothman (UBC FOM Digital Solutions: Ed Tech)
Edited by:
Stephen Gillis
Produced by UBC FOM Digital Solutions EdTech team facilitates innovation by UBC Medicine learners and faculty.
Website: https://education.med.ubc.ca/
Subscribe: https://www.youtube.com/ubcmed....vid?sub_confirmation
UBCMLN Podcast Network: https://tinyurl.com/ubcmedicinelearningnetwork
----------------------------------------------------------------------------------------------------------------------------------------------------------
The Vancouver Fraser Medical Program and the Vancouver Academic Campus of the University of British Columbia are situated on the traditional territory of the Musqueam, Squamish and Tsleil-Waututh peoples.
The Southern Medical Program and the Okanagan Academic Campus of the University of British Columbia are situated on the territory of the Syilx Okanagan Nation.
The Northern Medical Program and the University of Northern BC are situated on the traditional territory of the Lheidli T’enneh, part of the Dakelh (Carrier) First Nations.
With respect the Lekwungen peoples on whose traditional territory the Island Medical Program and the University of Victoria stand and the Songhees, Esquimalt and WSÁNEĆ peoples whose historical relationships with the land continue to this day.
We acknowledge our traditional hosts and honour their welcome and graciousness to the students who seek knowledge here.
© UBC Faculty of Medicine
All rights reserved. Reproduction and distribution of this presentation without written permission from UBC Faculty of Medicine is strictly prohibited.
Vitiligine News, Vitiligine Foto, Vitiligine Come Si Manifesta, La Vitiligine, Rimedi Vitiligine --- http://vitiligine-cura.good-info.co --- Non Importa Quanto Sia Grave La Tua Vitiligine, Puoi Iniziare A Utilizzare Questo Sistema Potente PROPRIO ORA Per Ottenere La Libertà Dalla Vitiligine Che Hai Sempre Sognato! Funziona In Tutti I Casi Seguenti: Vitiligine Leggera, Moderata O Grave Vitiligine Focale Vitiligine Segmentale Vitiligine Mucoidale Vitiligine acrofacciale Vitiligine vulgaris Vitiligine universale I trattamenti anti-vitiligine che la maggior parte della gente usa NON FUNZIONANO! Il 95% di tutti quelli che trattano la vitiligine finisce peggio di quando ha iniziato! Una Presentazione Video Gratuita Spiega Un Singolare Consiglio Per Eliminare La Vitiligine Per Sempre http://vitiligine-cura.good-info.co
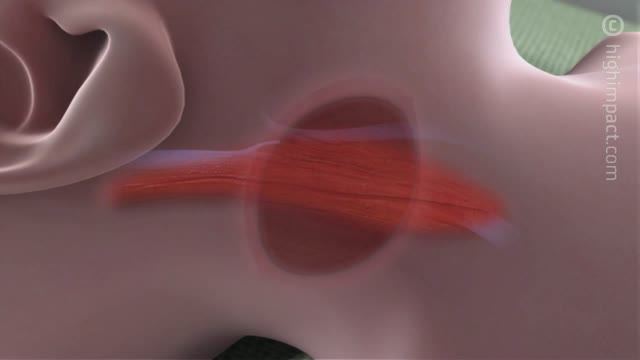
Central catheters provide dependable intravenous access and enable hemodynamic monitoring and blood sampling [1-3]. The jugular veins are one of the most popular sites for central venous access due to accessibility and overall low complication rates, and are the preferred site for temporary hemodialysis.
Integrative Physical Examination Lecture
A central venous catheter, also called a central line, is a long, thin, flexible tube used to give medicines, fluids, nutrients, or blood products over a long period of time, usually several weeks or more. A catheter is often inserted in the arm or chest through the skin into a large vein.

Dr. Linder is removing a patients breast implants after having five breast augmentations from three previous surgeons. She has baker 4 capsular contracture and is look forward to having them removed. The most common reasons for removing a breast implant include; heath reasons such as back pain, reoccurring complications and the desire for a different shape or size. For implant removal surgery, Dr. Linder makes an inframammary incision (along the breast crease). The implant can be removed intact, or it may need to be punctured before removal. An antibiotic solution is used to irrigate the breast pocket after implant removal. For more information about breast implant removal go to www.implantremoval.net or call Dr. Linder's office at 310-275-4513

A doctor pops a giant cyst on a boy's eye and films the whole thing. As the big cyst pops, puss oozes out.

SPIDER Surgery-- Single Incision Gallbladder Removal

Pulmonary edema is almost always treated in the emergency room or hospital. You may need to be in an intensive care unit (ICU). Oxygen is given through a face mask or tiny plastic tubes are placed in the nose. A breathing tube may be placed into the windpipe (trachea) so you can be connected to a breathing machine (ventilator) if you cannot breathe well on your own. The cause of edema should be identified and treated quickly. For example, if a heart attack has caused the condition, it must be treated right away. Medicines that may be used include: Diuretics that remove excess fluid from the body Medicines that strengthen the heart muscle, control the heartbeat, or relieve pressure on the heart
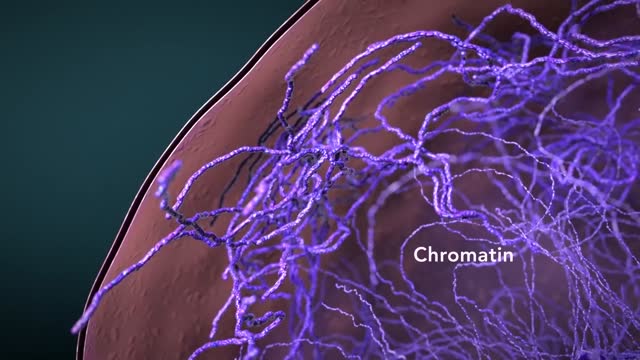
Cytoplasmic organelles are "little organs" that are suspended in the cytoplasm of the cell. Each type of organelle has a definite structure and a specific role in the function of the cell. Examples of cytoplasmic organelles are mitochondrion, ribosomes, endoplasmic reticulum, golgi apparatus, and lysosomes.
