- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Tonsil stones are hard yellow or white formations that are located on or within the tonsils. It’s common for people with tonsil stones to not even realize they have them. Tonsil stones aren’t always easily visible and they can range from rice- to pea-sized. Tonsil stones rarely cause larger health complications. However, sometimes they can grow into larger tonsilloliths which can cause your tonsils to swell

Most women have vaginal discharge at many different times throughout their cycle. During ovulation, white and watery discharge is common and accepted as normal. But, discharge after ovulation is widely believed to be a sign of pregnancy.

SUBSCRIBE: https://www.youtube.com/c/TVNe....phrologist?sub_confi
An animation of blood flow inside the Hemodialysis circuit.
About Dr. Rifai:
Dr. Ahmad Oussama Rifai is certified by the American Board of Internal Medicine (ABIM) in the specialty of Internal Medicine and the sub-specialty of Nephrology.
MEET DR. RIFAI
https://www.thevirtualnephrologist.com/rifai/
Follow The Virtual Nephrologist on SOCIAL MEDIA:
-Facebook: https://www.facebook.com/thevirtualnephrologist
-Instagram: https://www.instagram.com/thevirtualnephrologist/
-Twitter: https://twitter.com/VNephrologist
Schedule a virtual consult:
https://www.thevirtualnephrolo....gist.com/schedule-a-
Best wishes for great health | The Virtual Nephrologist

Scrubbing of Surgical Hands

A video showing breast examination after breast implants
This video demonstrates how to perform a cardiovascular examination in an OSCE station.
You can access our step-by-step OSCE guide to accompany this video here: https://geekymedics.com/cardio....vascular-examination
Check out our other awesome clinical skills resources including:
• 🔥 Geeky Medics Bundles (discounted products): https://app.geekymedics.com/purchase/bundles/
• ✨ 1000+ OSCE Stations: https://app.geekymedics.com/pu....rchase/osce-stations
• 🏥 Geeky Medics OSCE Revision Book: https://app.geekymedics.com/purchase/book/
• 📝 150+ PDF OSCE Checklists: https://geekymedics.com/pdf-osce-checklists/
• 🗂️ 3000+ OSCE Flashcards: https://app.geekymedics.com/pu....rchase/flashcard-col
• 📱 Geeky Medics OSCE App: https://geekymedics.com/geeky-medics-app/
• 🩺 Medical Finals SBA Question Pack: https://app.geekymedics.com/pu....rchase/medical-stude
• 💊 PSA Question Pack: https://app.geekymedics.com/pu....rchase/prescribing-s
Chapters:
- Introduction 00:00
- General inspection 00:35
- Hands 00:46
- Schamroth's window test 01:07
- Capillary refill 01:27
- Pulses 01:35
- Carotid auscultation 02:21
- Carotid pulse 02:43
- Jugular venous pressure 02:55
- Hepatojugular reflux 03:09
- Inspection of the face 03:21
- Inspection of the chest 03:49
- Apex beat 04:12
- Heaves and thrills 04:28
- Heart valve ausculation 04:49
- Accentuation manoeuvres 05:45
- Lung base auscultation 06:23
- Sacral and pedal oedema 06:43
- Summary 07:10
Subscribe to our newsletter to be the first to know about our latest content: https://geekymedics.com/newsletter/ ✉️
Join the Geeky Medics community: 👩👩👧👧
Twitter: http://www.twitter.com/geekymedics
Instagram: https://instagram.com/geekymedics
Facebook: http://www.facebook.com/geekymedics
Always adhere to your medical school/local hospital guidelines when performing examinations or clinical procedures. DO NOT perform any examination or procedure on patients based purely upon the content of these videos. Geeky Medics accepts no liability for loss of any kind incurred as a result of reliance upon the information provided in this video.
Normal heart sounds and aortic regurgitation/stenosis sounds
Recorded on a Thinklabs Digital Stethoscope (https://www.thinklabs.com)
Some people have found this video useful for ASMR purposes.
Symptoms of liver failure include vomiting, diarrhea and fatigue as well as the symptoms from stage 3. While the progression from cirrhosis to failure can take years, the damage is irreversible and leads to eventual death. The key to treating liver disease is to diagnose the condition as early as possible.

A pneumothorax occurs when some of the tiny air sacs (alveoli) in a baby's lung become overinflated and burst. This causes air to leak into the space between the lung and chest wall (pleural space). The most common cause of pneumothorax is respiratory distress syndrome. This is a condition that occurs in babies who are born too early (premature). The baby's lungs lack the slippery substance (surfactant) that helps them stay open. Therefore, the tiny air sacs are not able to expand as easily. If the baby is put on a breathing machine (mechanical ventilator), there is extra pressure on the baby's lungs, which can sometimes burst the air sacs.

This video is showing the Femoral Nerve Block

Most C-sections are done under regional anesthesia, which numbs only the lower part of your body — allowing you to remain awake during the procedure. A common choice is a spinal block, in which pain medication is injected directly into the sac surrounding your spinal cord

Leading cardiologists Valentin Fuster, MD, PhD, Director of Mount Sinai Heart and Herschel Sklaroff, MD, Clinical Professor of Medicine, Cardiology at Mount Sinai Heart were filmed for one-month for the “Making Rounds” documentary film as they cared for critically-ill heart patients in the Cardiac Care Unit at The Mount Sinai Hospital.
Watch Mount Sinai Heart doctors, fellows, residents, and nurses in action and saving lives demonstrating how simply listening to patients at the bedside remains medicine’s most indispensable tool over any technology.
In this film Mount Sinai Heart helps preserve the disappearing art and science of how to examine and diagnose patients at the bedside for future generations of physicians.
**This film was made possible by the generous support
of the McInerney Family.**
Copyright 2015 Middlemarch Films, Inc

In this video, I have covered Inguinal hernia under the following headings: Definition, Parts of Hernia, Surgical anatomy, Types of inguinal hernia, Aetiology of hernia, Clinical features of hernia, complications of hernia, Clinical examination, Surgical principles, and explanation of a few surgeries (Herniotomy, Bassini suture repair, Shouldice repair, Lichtenstein tension-free open meshplasty, hernia plugs, Laparoscopic techniques like TEP(Totally extraperitoneal approach) and TAPP(Transabdominal preperitoneal approach) surgical procedures).
SUBSCRIBE FOR MORE VIDEOS!
How to study General Surgery in med school: (Tips and Tricks)
https://youtu.be/_tad4i2Kdes
1-minute hernia videos: (Complete playlist by Skeleton)
https://www.youtube.com/watch?v=GsmAPYMiK_s&list=PL-dMZTUxuTxAi7rFqOy9o0pv1g-aZ1GXz
(includes femoral hernia, obturator hernia, epigastric hernia, umbilical hernia, Spigelian hernia, Richter hernia, lumbar hernia, incisional hernia, Hiatal hernia, congenital diaphragmatic hernia, contents of spermatic cord, triangles of hernia)
Study with me:
https://www.youtube.com/watch?v=lBkmmYcUBDo&t=291s
Hydrocele video:
https://www.youtube.com/watch?v=s6ICxMMtpYk&t=65s
You can support my channel by buying me a coffee here:
https://www.buymeacoffee.com/medvids
(Lecture slides will be available in the "EXTRAS" section of this link)
Instagram: @medvidsmadesimple
Check out my other works: linktr.ee/doctorcool

Robotic-assisted endoscopic thyroid surgery using the daVinci® Surgical System can safely and effectively offer those needing thyroid surgery relief without neck incisions. Dr. Ron Kuppersmith and Dr. Andrew deJong are now performing this procedure at the College Station Medical Center in Texas.

Vetical Mattress Suture

Interlocking Continuous Suture

New Minimally Invasive Procedure with No Pain or Downtime… From Dr. Michael Goodman, Caring For Women Wellness Center Laser Vaginal Tightening for Improved Sexual Pleasure and Relief from Minimal Urinary Incontinence Laser Vaginal Therapy for reversing Vaginal Atrophy (Good also for Breast Cancer Survivors with Vaginal Atrophy)

Delayed puberty is defined as the absence of any signs suggestive of puberty by 14 years of age. In this case, the patient's pubertal delay appears to be constitutional because of his positive family history, absence of syndromic features or systemic illness, and bone age of 12 years. Puberty correlates more closely with bone age than chronological age. On follow-up, the patient will most likely demonstrate a similar onset of puberty as his father.
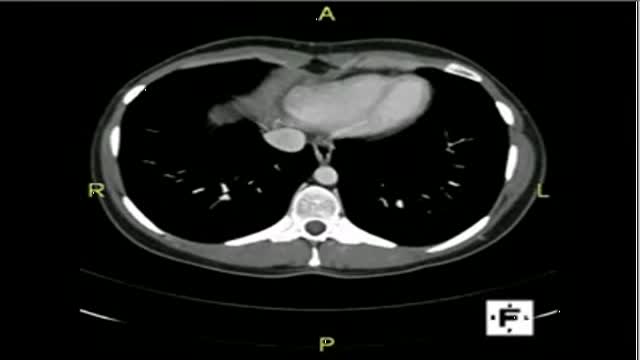
The video will describe anatomical structures as seen on a CT scan. Please see discalimer on my website.

💪 Get our Knee Resilience program here: https://e3rehab.com/programs/r....esilience/knee-resil
In this video, I will walk you through a comprehensive rehab program for the most commonly injured knee ligament - the MCL.
💪 PROGRAMS: https://e3rehab.com/programs/
📩 MAILING LIST (exclusive deals, offers, and information): https://e3rehab.com/newsletter/
🏆 COACHING: https://e3rehab.com/coaching/
📝 ARTICLES: https://e3rehab.com/articles/
👕 APPAREL: https://e3rehab.com/clothing/
🎧 PODCAST: https://open.spotify.com/show/....5ZbaI145Bk94Guq7olMJ
AFFILIATES:
👟 Vivo Barefoot: Get 15% off all shoes! - https://www.vivobarefoot.com/e3rehab
📓 MASS (Monthly Research Review): http://bit.ly/E3MASS
📚 CSMi: https://humacnorm.com/e3rehab
🏋️ GYM EQUIPMENT: https://e3rehab.com/affiliates/
Follow Us:
YOUTUBE: https://www.youtube.com/@e3reh....ab?sub_confirmation=
INSTAGRAM: https://www.instagram.com/e3rehab
TWITTER: https://twitter.com/E3Rehab
FACEBOOK: https://www.facebook.com/e3rehab
TIKTOK: https://www.tiktok.com/@e3rehab
Intro (0:00)
Anatomy & Function (0:08)
Classification (1:11)
Treatment Options (1:46)
Bracing (3:30)
Rehab Overview (4:28)
Early Stage (5:27)
Mid-Stage(8:50)
Late Stage/Return to Sport (21:14)
Programming (22:13)
Summary (23:47)
---
Disclaimer: The information presented is not intended as medical advice or to be a substitute for medical counseling but intended for entertainment purposes only. If you are experiencing pain, please seek the appropriate healthcare professional.

Watch this video to learn how and when to change a dressing for a child with a hemodialysis catheter. You should change your child's dressing if it becomes soiled with water or blood or if it comes off at home. Keeping a clean dressing on your child will limit risk of infection.
