- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
A central venous catheter, also called a central line, is a long, thin, flexible tube used to give medicines, fluids, nutrients, or blood products over a long period of time, usually several weeks or more. A catheter is often inserted in the arm or chest through the skin into a large vein.

SPIDER Surgery-- Single Incision Gallbladder Removal

"I’m essentially taking care of the baby right now to give them 60 or 70 or 80 years of life so I have to perform my best every time. Every single time. That is a commitment that I have to the parents."
The highest standard. That’s what cardiothoracic surgeon Sergio Carrillo demands of himself every time he steps into the OR. Dr. Carrillo and his Heart Center team at Nationwide Children’s Hospital treat patients with congenital heart disease with the simplest to the most complex procedures.
Connect with a specialist: http://bit.ly/2LU2kJn
The Heart Center at Nationwide Children's: http://bit.ly/2LTQmPR
Advancing cardiac care through research: http://bit.ly/2LXFqAD
Tissue Engineering Research & Innovation: http://bit.ly/2LUD0Ts
Heart & Chest Surgery, What to Expect: http://bit.ly/2LVQr5J
Meet our Heart Center Team: http://bit.ly/2LUvdF9
Vitiligine News, Vitiligine Foto, Vitiligine Come Si Manifesta, La Vitiligine, Rimedi Vitiligine --- http://vitiligine-cura.good-info.co --- Non Importa Quanto Sia Grave La Tua Vitiligine, Puoi Iniziare A Utilizzare Questo Sistema Potente PROPRIO ORA Per Ottenere La Libertà Dalla Vitiligine Che Hai Sempre Sognato! Funziona In Tutti I Casi Seguenti: Vitiligine Leggera, Moderata O Grave Vitiligine Focale Vitiligine Segmentale Vitiligine Mucoidale Vitiligine acrofacciale Vitiligine vulgaris Vitiligine universale I trattamenti anti-vitiligine che la maggior parte della gente usa NON FUNZIONANO! Il 95% di tutti quelli che trattano la vitiligine finisce peggio di quando ha iniziato! Una Presentazione Video Gratuita Spiega Un Singolare Consiglio Per Eliminare La Vitiligine Per Sempre http://vitiligine-cura.good-info.co

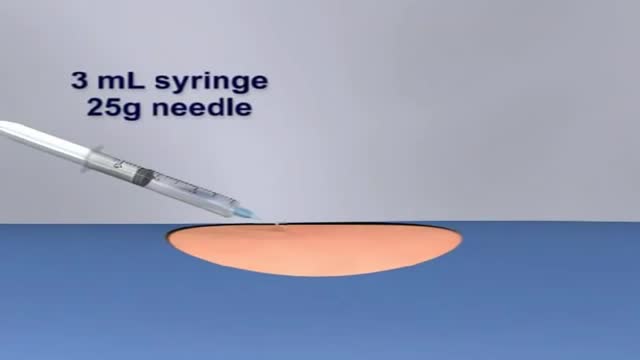
Thoracentesis is a minimally invasive procedure used to diagnose and treat pleural effusions, a condition in which there is excess fluid in the pleural space, also called the pleural cavity. This space exists between the outside of the lungs and the inside of the chest wall.
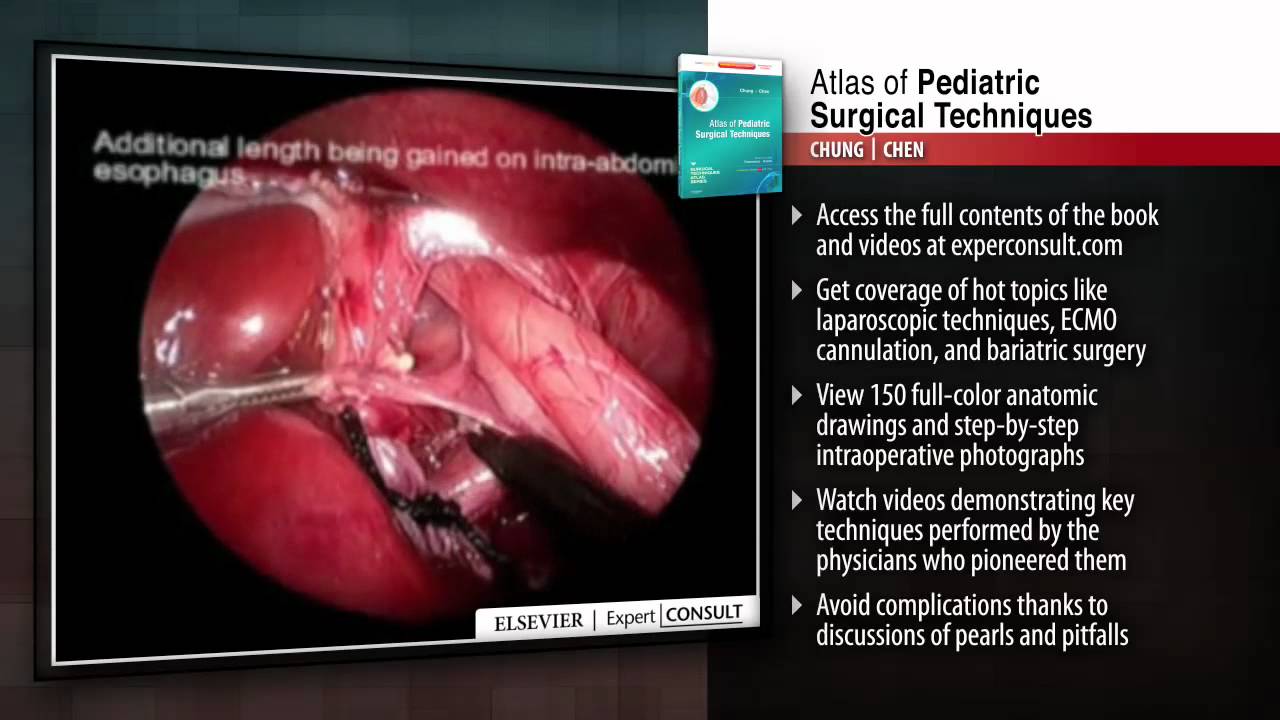
This title in the new Surgical Techniques Atlas series presents state-of-the-art updates on the full range of pediatric surgical techniques performed today. Expand your repertoire and hone your clinical skills thanks to the expert advice, procedural videos, and online access at expertconsult.com. For more information, please visit http://www.us.elsevierhealth.com/product.jsp?sid=EHS_US_BS-SPE-59&isbn=9781416046899&dmnum=null&elsca1=CriticalCare&elsca2=soc_med&elsca3=null&elsca4=youtube_ELSpromovideos

It depends upon which ligament is injured. If it is medial collateral ligament you feel pain when you walk ,sit and stand and you will be liming as well. If it is anterior cruciate ligament you feel pain when you walk on uneven ground.

Watch that Full Real Human Body Decomposition Process
You've come to the perfect YouTube Video if you want to learn hospital and medical English while watching shows of "The Good Doctor." Watch medical English talks from the TV show "the good doctor" to acquire new terminology about ailments that people experience but don't know the names of.
Medical English Lesson 2 with the good doctor - https://youtu.be/gU107Q9Jerw
Hospital English Vocabulary Lesson 3 with Dr. House - https://youtu.be/lE4i1pY53Us
Illness English used in Hospitals Lesson 4 with Chicago Med - https://youtu.be/u3VPRdierKA
So keep learning and watching our video lessons to learn and improve your English to a great level.
Other English lessons through The Big Bang Theory
Learn English through Big Bang Theory Lesson 1 - https://youtu.be/iM-o5EKK5pg
Funny English Lesson through Big Bang Theory Lesson 2 - https://youtu.be/O6CRNi6OJ1k
Enjoy Learning English through Big Bang Theory Lesson 3 - https://youtu.be/-iSDlbReAxk
Want to Learn English through Big Bang Theory Lesson 4 - https://youtu.be/AZSkyjk-Ioo
Learn Romantic English with The Big Bang Theory - Lesson 5 - https://youtu.be/k5EqRArT41w
Visit our Instagram page: https://www.instagram.com/englishfluencymission/
Our Facebook Page: https://www.facebook.com/englishfluencymission/
To be fluent in English, we should have a vocabulary of between 3000 and 4000 important English words. Once we attain this objective, we can be guaranteed to sound like a native speaker.
The links to a few books I've collected for you are listed below; if you truly enjoy, these could be excellent starting points for your quest for greater English fluency.
Oxford Learner's Pocket Word Skills: Pocket-sized, topic-based English vocabulary - https://amzn.to/34LKv7a
Word power made easy - https://amzn.to/38Ht8Fy
Cambridge Grammar for IELTS - https://amzn.to/34OUdWa
Unbroken - The incredible true story of Louis Zamperini, now a major motion picture directed by Angelina Jolie. - https://amzn.to/3rqtyZH
THE INTERNATIONAL NUMBER ONE BESTSELLER -
Other Video Lessons:
Learn English with Wonder Woman - https://youtu.be/6F8oqQWErU0
Learn English with Stuart Little - https://youtu.be/EIeOooR8vas
Learn English with Avengers 2012 - https://youtu.be/u97FZWkd4A8
Learn English with Forrest Gump - https://youtu.be/uH_kTF8QAZc
Learn English with Spider-Man 2 (2004) - https://youtu.be/DHy-2g-N7SQ
Your Queries
learn English with movies
learning English from movies
English vocabulary through Hollywood movies
hospital English conversation
hospital English words
hospital English movie
hospital English video
hospital English vocabulary
hospital English speaking
hospital English sentences
medical English speaking practice
medical English conversation
medical English words
medical English listening practice with the good doctor
learn hospital English with the good doctor
#thegooddoctor #learnenglishwithtvseries
What is peripheral neuropathy? Your peripheral nervous system connects the nerves from your brain and spinal cord, or central nervous system, to the rest of your body. This includes your: arms hands feet legs internal organs mouth face The job of these nerves is to deliver signals about physical sensations back to your brain.

A Beautiful Smile at Lake Pointe is Sugar Land premier dentistry practice. Dr. Lance Jue has been serving patients' preventive, restorative and cosmetic dental needs here in Sugar Land for over 19 years. Book an appointment online now with Dr. Lance Jue


A pneumothorax can be caused by a blunt or penetrating chest injury, certain medical procedures, or damage from underlying lung disease. Or it may occur for no obvious reason. Symptoms usually include sudden chest pain and shortness of breath. On some occasions, a collapsed lung can be a life-threatening event.

Arm Replantation of a Child By Dr. Omid Liaghat : https:drliaghatclinic.com

Sexual Desire & our Eating

Watch to learn more about what happens during a stent procedure.
More information about this procedure and other heart care at BJC: https://www.bjc.org/Services/M....edical-Services/angi

Watch that video of a Terrible Bodybuilder's Colon Contains 10 lbs of Meat Worms

49-years old patient complaining of cough, fever and pleuritic pain for 2 weeks. At admission he was febrile and tachypnic. Chest X-Ray showed left pleural effusion. Thoracocentesis revealed purulent fluid. Chest CT-scan showed large and loculated left pleural effusion and pleural thickening. VATS decortication was performed through three incisions.
