- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A vide showing how to introduce an arteral catheter

Hip Dislocation Reduction

Bone Marrow Aspiration

Breast Massage Technique For Good Breast Health

Female ejaculation is characterized as an expulsion of fluid from or near the vagina during or before an orgasm

Endoscopic Carpal Tunnel Release Surgery
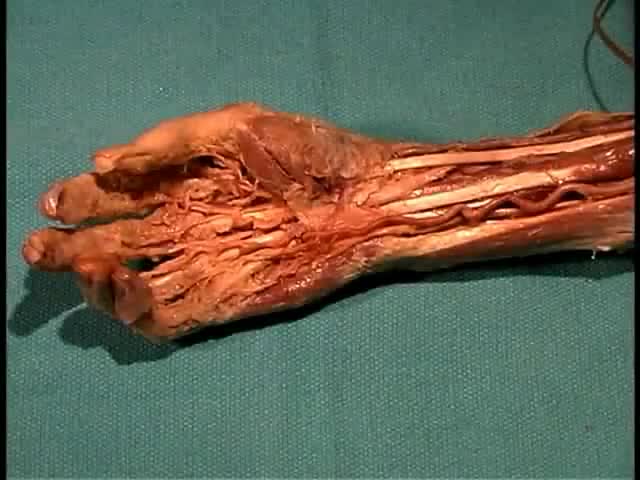
Anatomy of The Forearm and Hand
Thalassemia (thal-uh-SEE-me-uh) is an inherited blood disorder characterized by less hemoglobin and fewer red blood cells in your body than normal. Several types of thalassemia exist, including alpha-thalassemia, beta-thalassemia intermedia, Cooley's anemia and Mediterranean anemia. Hemoglobin is the substance in your red blood cells that allows them to carry oxygen. The low hemoglobin and fewer red blood cells of thalassemia may cause anemia, leaving you fatigued. If you have mild thalassemia, you may not need treatment. But, if you have a more severe form of thalassemia, you may need regular blood transfusions. You can also take steps on your own to cope with fatigue, such as choosing a healthy diet and exercising regularly.
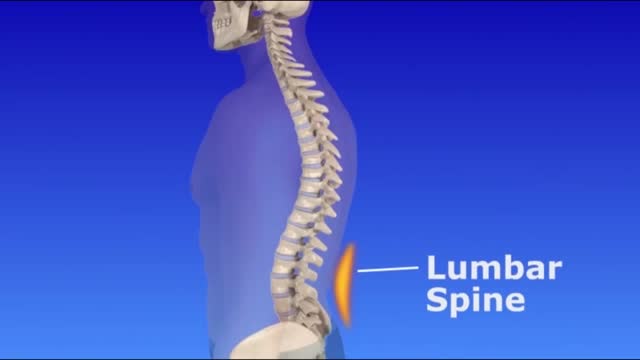
If you look at someone’s back, you’ll see that the spine runs straight down the middle. When a person has scoliosis, their backbone curves to the side. The angle of the curve may be small, large or somewhere in between. But anything that measures more than 10 degrees is considered scoliosis. Doctors may use the letters “C” and “S” to describe the curve of the backbone. You probably don’t look directly at too many spines, but what you might notice about someone with scoliosis is the way they stand. They may lean a little or have shoulders or hips that look uneven. What Causes Scoliosis? In as many as 80% of cases, doctors don’t find the exact reason for a curved spine. Scoliosis without a known cause is what doctors call “idiopathic.” Some kinds of scoliosis do have clear causes. Doctors divide those curves into two types -- structural and nonstructural. In nonstructural scoliosis, the spine works normally, but looks curved. Why does this happen? There are a number of reasons, such as one leg’s being longer than the other, muscle spasms, and inflammations like appendicitis. When these problems are treated, this type of scoliosis often goes away.

Continuous Connell Pattern Suture
Migraine
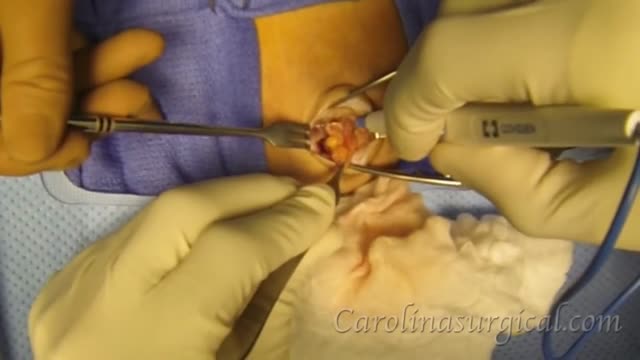
Inguinal hernia repair is surgery to repair a hernia in your groin. A hernia is tissue that bulges out of a weak spot in the abdominal wall. Your intestine may bulge out through this weakened area.Mar 13, 2015
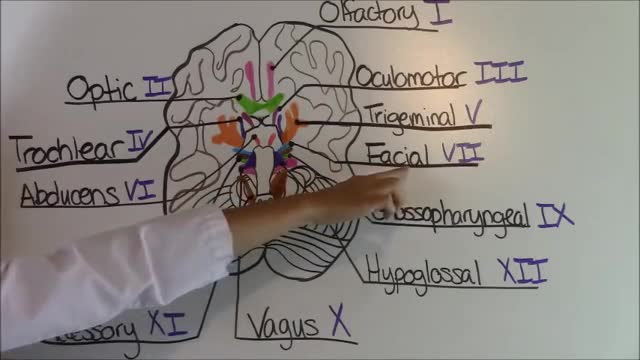
Cranial Nerves Mnemonic
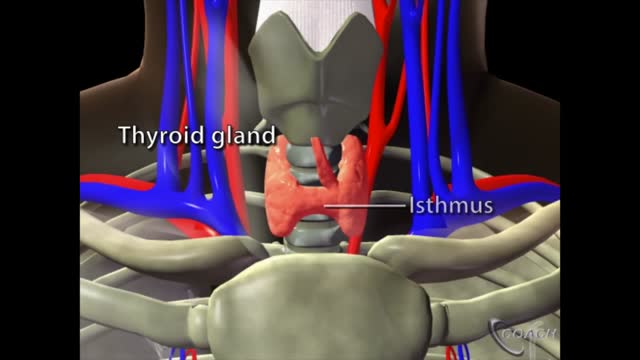
The thyroid is a butterfly-shaped gland that sits low on the front of the neck. Your thyroid lies below your Adam’s apple, along the front of the windpipe. The thyroid has two side lobes, connected by a bridge (isthmus) in the middle. When the thyroid is its normal size, you can’t feel it.

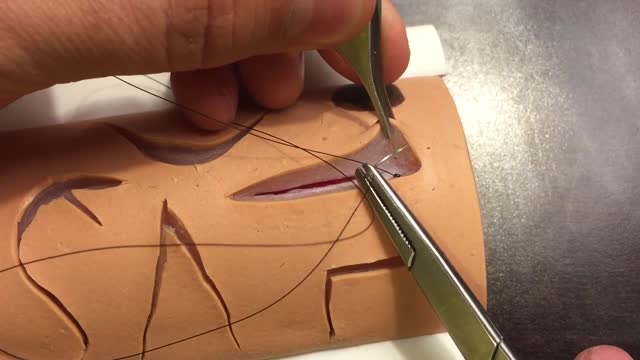
A very good video illustrating the Interrupted Sub-Dermal Sutures

Inspection of the neck
The two biggest considerations when choosing a suture are the location and tension of the wound. Other important considerations are tensile strength, knot strength, handling, and tissue reactivity. Sutures are divided into two major groups: Absorbable – lose the majority of their tensile strength in less than 60 days. They are generally used for buried sutures and do not require removal. Non-absorbable – maintain the majority of their tensile strength for more than 60 days. They are generally used for skin surface sutures and do require removal postoperatively. Suture needles also come in a variety of shapes and sizes. Curved needles are almost exclusively used in dermatological surgery. Cutting needles move through the tissue more easily and may have their primary cutting edge on the inside of the curve (conventional cutting) or outside of the curve (reverse cutting). The benefit of reverse cutting is that the tapered puncture left by the suture is directed away from the wound edge and therefore tissue tearing is less common. Non-cutting round needles cause even less tissue tearing and may be especially useful in delicate areas and fascia.
Carpal tunnel syndrome is a common condition that causes pain, numbness, and tingling in the hand and arm. The condition occurs when one of the major nerves to the hand — the median nerve — is squeezed or compressed as it travels through the wrist. In most patients, carpal tunnel syndrome gets worse over time, so early diagnosis and treatment are important. Early on, symptoms can often be relieved with simple measures like wearing a wrist splint or avoiding certain activities. If pressure on the median nerve continues, however, it can lead to nerve damage and worsening symptoms. To prevent permanent damage, surgery to take pressure off the median nerve may be recommended for some patients.

Use of Skin Stapler
Lung inflation and pleural membranes anatomy
