- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

To learn more about licensing this video for content marketing or patient education purposes, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=hiv-112513
This video, created by Nucleus Medical Media, shows the function of white blood cells in normal immunity. It also portrays how the human immunodeficiency virus (HIV) affects the immune system and causes acquired immunodeficiency syndrome (AIDS). Common types of antiretroviral medications used to treat HIV and AIDS are also shown.
#HIV #AIDS #HumanImmunodeficiencyVirus
ANH13111

A pneumothorax occurs when some of the tiny air sacs (alveoli) in a baby's lung become overinflated and burst. This causes air to leak into the space between the lung and chest wall (pleural space). The most common cause of pneumothorax is respiratory distress syndrome. This is a condition that occurs in babies who are born too early (premature). The baby's lungs lack the slippery substance (surfactant) that helps them stay open. Therefore, the tiny air sacs are not able to expand as easily. If the baby is put on a breathing machine (mechanical ventilator), there is extra pressure on the baby's lungs, which can sometimes burst the air sacs.

This video is showing the Femoral Nerve Block

What is an ingrown hair cyst? An ingrown hair cyst refers to an ingrown hair that turns into a cyst — a large bump that extends between the skin’s surface and deep underneath it. The appearance is a cross between a regular ingrown hair and an acne cyst, though this is a different condition. These types of cysts are common among people who shave, wax, or use other methods to remove their hair. Although you may be eager to get rid of these cysts simply because of their appearance, it’s also important to watch for signs of an infection. Keep reading to learn what causes these cysts to form, plus how to treat them and prevent them from returning.

Most women have vaginal discharge at many different times throughout their cycle. During ovulation, white and watery discharge is common and accepted as normal. But, discharge after ovulation is widely believed to be a sign of pregnancy.

In this video, I have covered Inguinal hernia under the following headings: Definition, Parts of Hernia, Surgical anatomy, Types of inguinal hernia, Aetiology of hernia, Clinical features of hernia, complications of hernia, Clinical examination, Surgical principles, and explanation of a few surgeries (Herniotomy, Bassini suture repair, Shouldice repair, Lichtenstein tension-free open meshplasty, hernia plugs, Laparoscopic techniques like TEP(Totally extraperitoneal approach) and TAPP(Transabdominal preperitoneal approach) surgical procedures).
SUBSCRIBE FOR MORE VIDEOS!
How to study General Surgery in med school: (Tips and Tricks)
https://youtu.be/_tad4i2Kdes
1-minute hernia videos: (Complete playlist by Skeleton)
https://www.youtube.com/watch?v=GsmAPYMiK_s&list=PL-dMZTUxuTxAi7rFqOy9o0pv1g-aZ1GXz
(includes femoral hernia, obturator hernia, epigastric hernia, umbilical hernia, Spigelian hernia, Richter hernia, lumbar hernia, incisional hernia, Hiatal hernia, congenital diaphragmatic hernia, contents of spermatic cord, triangles of hernia)
Study with me:
https://www.youtube.com/watch?v=lBkmmYcUBDo&t=291s
Hydrocele video:
https://www.youtube.com/watch?v=s6ICxMMtpYk&t=65s
You can support my channel by buying me a coffee here:
https://www.buymeacoffee.com/medvids
(Lecture slides will be available in the "EXTRAS" section of this link)
Instagram: @medvidsmadesimple
Check out my other works: linktr.ee/doctorcool

Detailed examination of the joints is usually not included in the routine medical examination. However, joint related complaints are rather common, and understanding anatomy and physiology of both normal function and pathologic conditions is critically important when evaluating the symptomatic patient. By gaining an appreciation for the basic structures and functioning of the joint, you'll be able to "logic" your way thru the exam, even if you can't remember the eponym attached to each specific test!

Robotic-assisted endoscopic thyroid surgery using the daVinci® Surgical System can safely and effectively offer those needing thyroid surgery relief without neck incisions. Dr. Ron Kuppersmith and Dr. Andrew deJong are now performing this procedure at the College Station Medical Center in Texas.

New Minimally Invasive Procedure with No Pain or Downtime… From Dr. Michael Goodman, Caring For Women Wellness Center Laser Vaginal Tightening for Improved Sexual Pleasure and Relief from Minimal Urinary Incontinence Laser Vaginal Therapy for reversing Vaginal Atrophy (Good also for Breast Cancer Survivors with Vaginal Atrophy)

Vetical Mattress Suture

Interlocking Continuous Suture

demonstrates how the Epley maneuver is performed to treat POSTERIOR canal BPPV affecting the right ear. Animation showing what is going on within the inner ear is also shown in the 2nd half of the video.
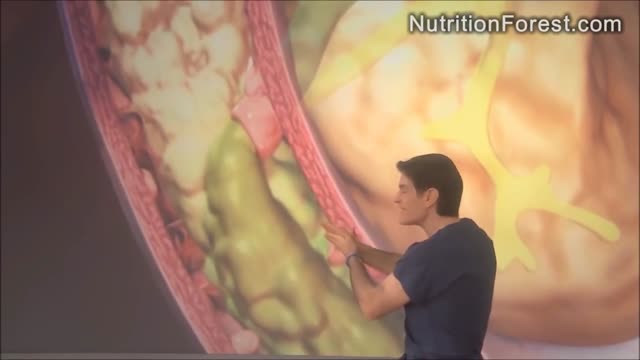
How To Cleanse Colon
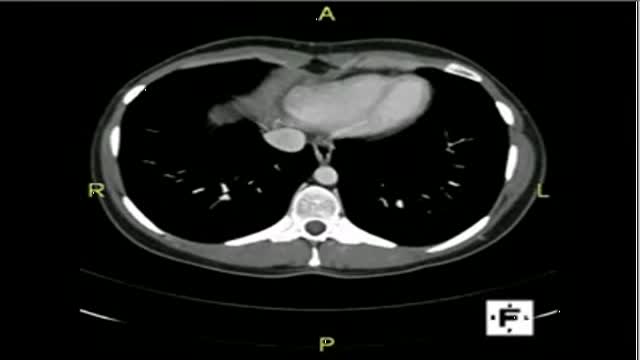
The video will describe anatomical structures as seen on a CT scan. Please see discalimer on my website.

The Epley maneuver or repositioning maneuver is a maneuver used to treat benign paroxysmal positional vertigo of the posterior or anterior canals

new study about the size of penis
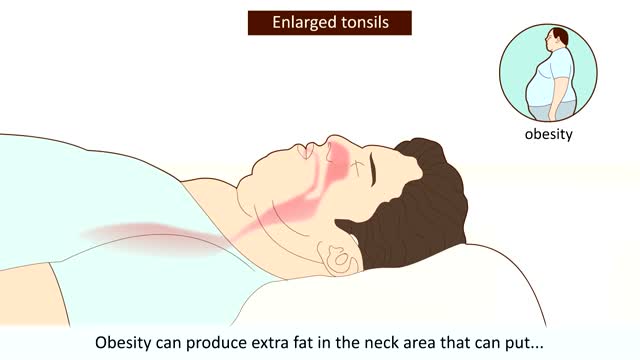
What Is Sleep Apnea? When you have this condition, your breath can become very shallow or you may even stop breathing -- briefly -- while you sleep. It can happen many times a night in some people. Obstructive sleep apnea happens when something partly or completely blocks your upper airway during shut-eye. That makes your diaphragm and chest muscles work harder to open the obstructed airway and pull air into the lungs. Breathing usually resumes with a loud gasp, snort, or body jerk. You may not sleep well, but you probably won't be aware that this is happening.
Brought to you by http://nursing-resource.com

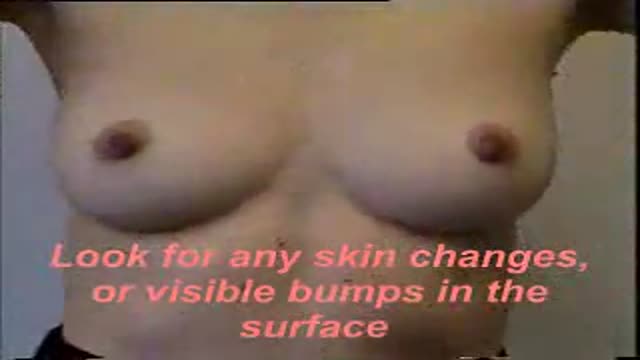
Identify the anatomy and explain the physiology of the breast on diagrams and sonograms.
Describe and demonstrate the protocol for sonographic scanning of the breast, including the clock and quadrant methods, and targeted examinations based on mammographic findings.
Describe the various diagnostic pathways that may lead to a sonographic breast examination, and explain how the ultrasound findings are correlated with other imaging modalities.
Identify and describe sonographic images of benign and malignant features and common breast pathologies.
Explain biopsy techniques for breast tumors.
Define and use related medical terminology.
Explain the Patient Privacy Rule (HIPAA) and Patient Safety Act (see reference

Our General Surgery team treats hernia patients on a daily basis. In fact, you could consider them to be hernia experts. We sat down with one of those experts, Dr. Heater Dunlap, to talk about the common signs and symptoms of hernias and to answer the question of when to see a doctor.
