- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
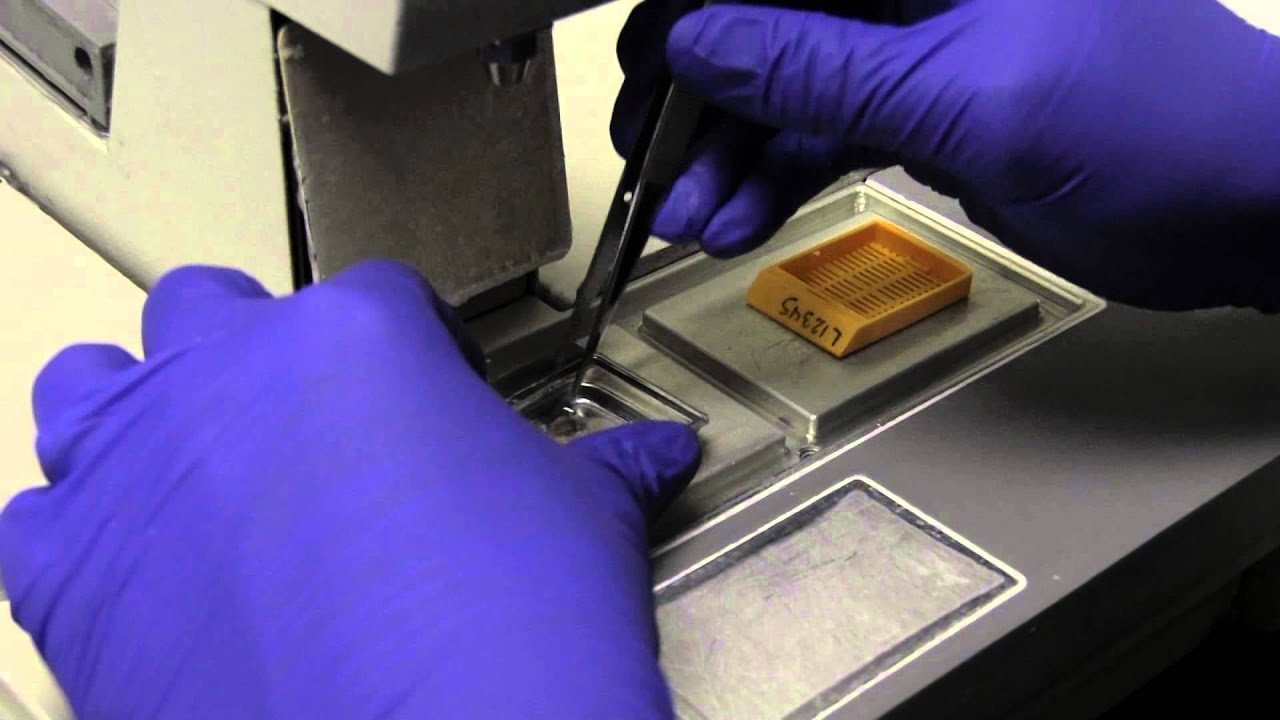
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

It depends upon which ligament is injured. If it is medial collateral ligament you feel pain when you walk ,sit and stand and you will be liming as well. If it is anterior cruciate ligament you feel pain when you walk on uneven ground.
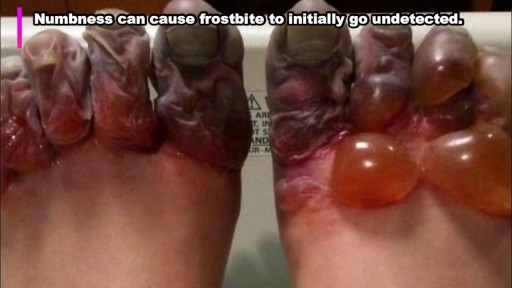
rostbite refers to the freezing of body tissue (usually skin) that results when the blood vessels contract, reducing blood flow and oxygen to the affected body parts. Normal sensation is lost, and color changes also occur in these tissues.

My baby is breech. Is it okay to get an external cephalic version (ECV)?
You've come to the perfect YouTube Video if you want to learn hospital and medical English while watching shows of "The Good Doctor." Watch medical English talks from the TV show "the good doctor" to acquire new terminology about ailments that people experience but don't know the names of.
Medical English Lesson 2 with the good doctor - https://youtu.be/gU107Q9Jerw
Hospital English Vocabulary Lesson 3 with Dr. House - https://youtu.be/lE4i1pY53Us
Illness English used in Hospitals Lesson 4 with Chicago Med - https://youtu.be/u3VPRdierKA
So keep learning and watching our video lessons to learn and improve your English to a great level.
Other English lessons through The Big Bang Theory
Learn English through Big Bang Theory Lesson 1 - https://youtu.be/iM-o5EKK5pg
Funny English Lesson through Big Bang Theory Lesson 2 - https://youtu.be/O6CRNi6OJ1k
Enjoy Learning English through Big Bang Theory Lesson 3 - https://youtu.be/-iSDlbReAxk
Want to Learn English through Big Bang Theory Lesson 4 - https://youtu.be/AZSkyjk-Ioo
Learn Romantic English with The Big Bang Theory - Lesson 5 - https://youtu.be/k5EqRArT41w
Visit our Instagram page: https://www.instagram.com/englishfluencymission/
Our Facebook Page: https://www.facebook.com/englishfluencymission/
To be fluent in English, we should have a vocabulary of between 3000 and 4000 important English words. Once we attain this objective, we can be guaranteed to sound like a native speaker.
The links to a few books I've collected for you are listed below; if you truly enjoy, these could be excellent starting points for your quest for greater English fluency.
Oxford Learner's Pocket Word Skills: Pocket-sized, topic-based English vocabulary - https://amzn.to/34LKv7a
Word power made easy - https://amzn.to/38Ht8Fy
Cambridge Grammar for IELTS - https://amzn.to/34OUdWa
Unbroken - The incredible true story of Louis Zamperini, now a major motion picture directed by Angelina Jolie. - https://amzn.to/3rqtyZH
THE INTERNATIONAL NUMBER ONE BESTSELLER -
Other Video Lessons:
Learn English with Wonder Woman - https://youtu.be/6F8oqQWErU0
Learn English with Stuart Little - https://youtu.be/EIeOooR8vas
Learn English with Avengers 2012 - https://youtu.be/u97FZWkd4A8
Learn English with Forrest Gump - https://youtu.be/uH_kTF8QAZc
Learn English with Spider-Man 2 (2004) - https://youtu.be/DHy-2g-N7SQ
Your Queries
learn English with movies
learning English from movies
English vocabulary through Hollywood movies
hospital English conversation
hospital English words
hospital English movie
hospital English video
hospital English vocabulary
hospital English speaking
hospital English sentences
medical English speaking practice
medical English conversation
medical English words
medical English listening practice with the good doctor
learn hospital English with the good doctor
#thegooddoctor #learnenglishwithtvseries

Sexual Desire & our Eating
What is peripheral neuropathy? Your peripheral nervous system connects the nerves from your brain and spinal cord, or central nervous system, to the rest of your body. This includes your: arms hands feet legs internal organs mouth face The job of these nerves is to deliver signals about physical sensations back to your brain.

Watch to learn more about what happens during a stent procedure.
More information about this procedure and other heart care at BJC: https://www.bjc.org/Services/M....edical-Services/angi
Shingles is a viral infection that causes a painful rash. Although shingles can occur anywhere on your body, it most often appears as a single stripe of blisters that wraps around either the left or the right side of your torso. Shingles is caused by the varicella-zoster virus — the same virus that causes chickenpox. After you've had chickenpox, the virus lies inactive in nerve tissue near your spinal cord and brain. Years later, the virus may reactivate as shingles. While it isn't a life-threatening condition, shingles can be very painful. Vaccines can help reduce the risk of shingles, while early treatment can help shorten a shingles infection and lessen the chance of complications.

The G-SHOT® (clinical description: G-Spot Amplification™ or GSA™), is a simple, nonsurgical, physician-administered treatment that can temporarily augment the Grafenburg spot (G-Spot) in sexually active women with normal sexual function.

Watch that video of Turning The Human Body to Ashes

Dr. Neel Joshi, Clinical Chief, Department of Surgery at Cedars Sinai, describes his technique for trocar removal at the end of laparoscopic cholecystectomy.
#medicaleducation #laparoscopicsurgery
Vaginal Hysterectomy Procedure of a 42 years old female patient with a 3 months history of symptomatic vaginal bulge
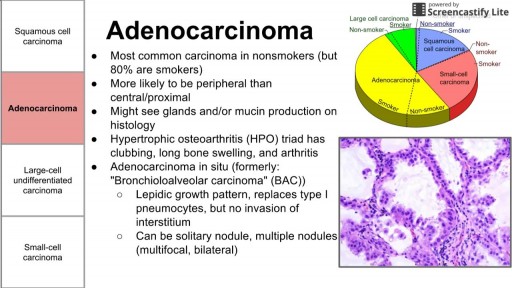
There are three main types of lung cancer. Knowing which type you have is important because it affects your treatment options and your outlook (prognosis). If you aren’t sure which type of lung cancer you have, ask your doctor so you can get the right information.
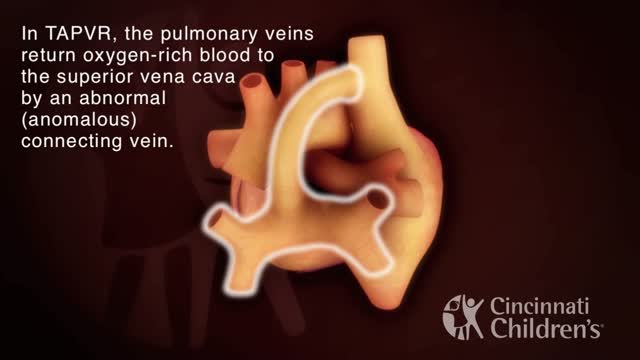
Total anomalous pulmonary venous return (TAPVR) is a rare congenital malformation in which pulmonary veins that return oxygen-rich blood from the lungs do not connect normally to the left atrium. Instead all four pulmonary veins drain abnormally to the right atrium. Heart models and animation were developed by the Cincinnati Children's Heart Institute in conjunction with Cincinnati Children's Critical Care Media Lab.

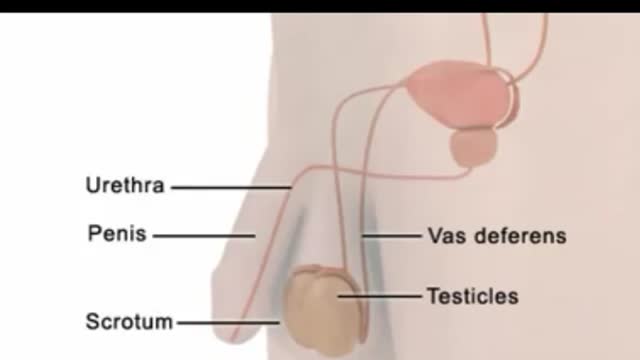
An egg cannot be fertilized when there are no sperm in the semen. The testicles continue to produce sperm, but the sperm are reabsorbed by the body. (This also happens to sperm that are not ejaculated after a while, regardless of whether you have had a vasectomy.) Sperm are made in the testicles. They pass through two tubes called the vasa deferentia to other glands and mix with seminal fluids to form semen. Vasectomy blocks each vas deferens and keeps sperm out of the seminal fluid. The sperm are absorbed by the body instead of being ejaculated.

James Dunn, MD, PhD is a pediatric surgeon at Stanford Children's Health. He is board certified in General Surgery and Pediatric Surgery.
Learn more at https://www.stanfordchildrens.....org/en/service/gener
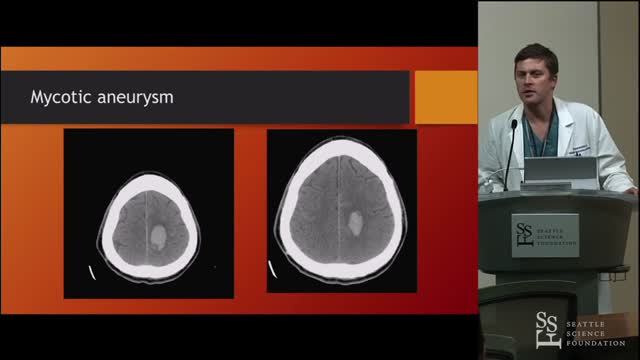
The headache, lethargy, and neck stiffness suggest subarachnoid hemorrhage secondary to rupture of a mycotic aneurysm. Mycotic or infected arterial aneurysms can develop due to metastatic infection from IE, with septic embolization and localized vessel wall destruction in the cerebral (or systemic) circulation. Intracerebral mycotic aneurysms can present as an expanding mass with focal neurologic findings or may not be apparent until aneurysm rupture with stroke or subarachnoid hemorrhage. The diagnosis of mycotic cerebral aneurysm can usually be confirmed with computed tomography angiography. Management includes broad-spectrum antibiotics (tailored to blood culture results) and surgical intervention (open or endovascular).
