- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This video is showing the Femoral Nerve Block
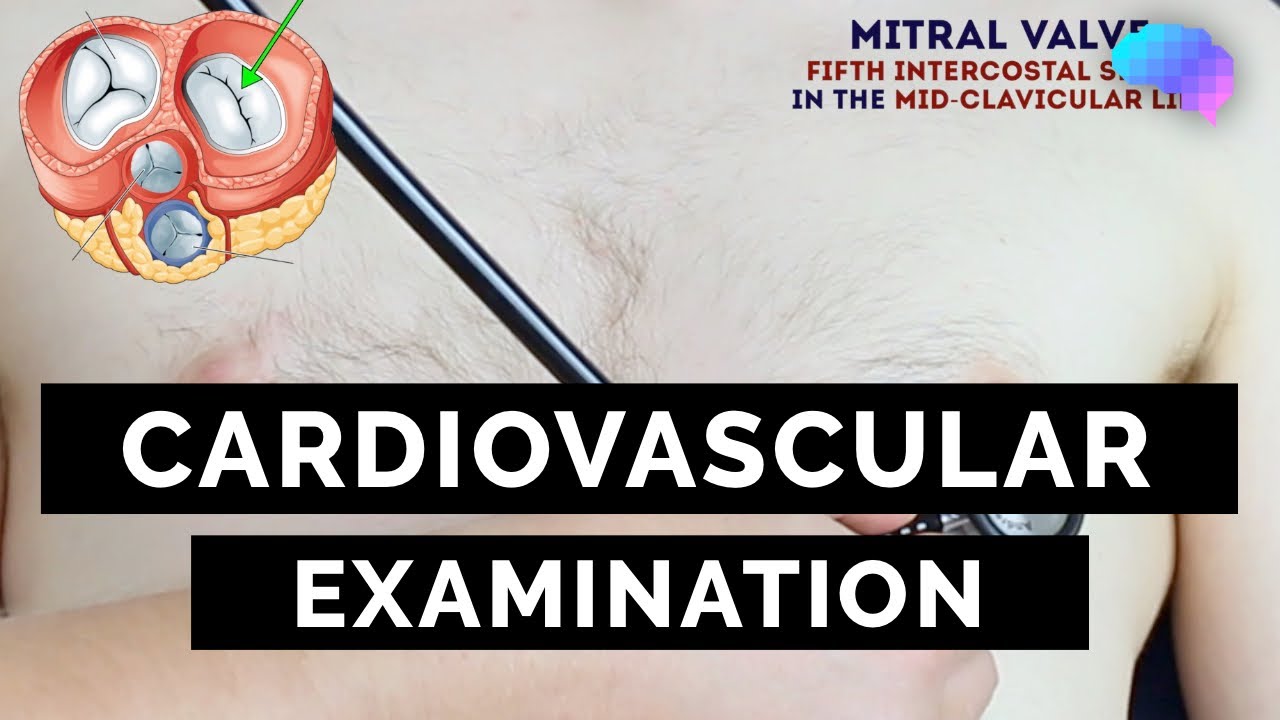
This video demonstrates how to perform a cardiovascular examination in an OSCE station.
You can access our step-by-step OSCE guide to accompany this video here: https://geekymedics.com/cardio....vascular-examination
Check out our other awesome clinical skills resources including:
• 🔥 Geeky Medics Bundles (discounted products): https://app.geekymedics.com/purchase/bundles/
• ✨ 1000+ OSCE Stations: https://app.geekymedics.com/pu....rchase/osce-stations
• 🏥 Geeky Medics OSCE Revision Book: https://app.geekymedics.com/purchase/book/
• 📝 150+ PDF OSCE Checklists: https://geekymedics.com/pdf-osce-checklists/
• 🗂️ 3000+ OSCE Flashcards: https://app.geekymedics.com/pu....rchase/flashcard-col
• 📱 Geeky Medics OSCE App: https://geekymedics.com/geeky-medics-app/
• 🩺 Medical Finals SBA Question Pack: https://app.geekymedics.com/pu....rchase/medical-stude
• 💊 PSA Question Pack: https://app.geekymedics.com/pu....rchase/prescribing-s
Chapters:
- Introduction 00:00
- General inspection 00:35
- Hands 00:46
- Schamroth's window test 01:07
- Capillary refill 01:27
- Pulses 01:35
- Carotid auscultation 02:21
- Carotid pulse 02:43
- Jugular venous pressure 02:55
- Hepatojugular reflux 03:09
- Inspection of the face 03:21
- Inspection of the chest 03:49
- Apex beat 04:12
- Heaves and thrills 04:28
- Heart valve ausculation 04:49
- Accentuation manoeuvres 05:45
- Lung base auscultation 06:23
- Sacral and pedal oedema 06:43
- Summary 07:10
Subscribe to our newsletter to be the first to know about our latest content: https://geekymedics.com/newsletter/ ✉️
Join the Geeky Medics community: 👩👩👧👧
Twitter: http://www.twitter.com/geekymedics
Instagram: https://instagram.com/geekymedics
Facebook: http://www.facebook.com/geekymedics
Always adhere to your medical school/local hospital guidelines when performing examinations or clinical procedures. DO NOT perform any examination or procedure on patients based purely upon the content of these videos. Geeky Medics accepts no liability for loss of any kind incurred as a result of reliance upon the information provided in this video.
Normal heart sounds and aortic regurgitation/stenosis sounds
Recorded on a Thinklabs Digital Stethoscope (https://www.thinklabs.com)
Some people have found this video useful for ASMR purposes.

In this video, I have covered Inguinal hernia under the following headings: Definition, Parts of Hernia, Surgical anatomy, Types of inguinal hernia, Aetiology of hernia, Clinical features of hernia, complications of hernia, Clinical examination, Surgical principles, and explanation of a few surgeries (Herniotomy, Bassini suture repair, Shouldice repair, Lichtenstein tension-free open meshplasty, hernia plugs, Laparoscopic techniques like TEP(Totally extraperitoneal approach) and TAPP(Transabdominal preperitoneal approach) surgical procedures).
SUBSCRIBE FOR MORE VIDEOS!
How to study General Surgery in med school: (Tips and Tricks)
https://youtu.be/_tad4i2Kdes
1-minute hernia videos: (Complete playlist by Skeleton)
https://www.youtube.com/watch?v=GsmAPYMiK_s&list=PL-dMZTUxuTxAi7rFqOy9o0pv1g-aZ1GXz
(includes femoral hernia, obturator hernia, epigastric hernia, umbilical hernia, Spigelian hernia, Richter hernia, lumbar hernia, incisional hernia, Hiatal hernia, congenital diaphragmatic hernia, contents of spermatic cord, triangles of hernia)
Study with me:
https://www.youtube.com/watch?v=lBkmmYcUBDo&t=291s
Hydrocele video:
https://www.youtube.com/watch?v=s6ICxMMtpYk&t=65s
You can support my channel by buying me a coffee here:
https://www.buymeacoffee.com/medvids
(Lecture slides will be available in the "EXTRAS" section of this link)
Instagram: @medvidsmadesimple
Check out my other works: linktr.ee/doctorcool

demonstrates how the Epley maneuver is performed to treat POSTERIOR canal BPPV affecting the right ear. Animation showing what is going on within the inner ear is also shown in the 2nd half of the video.

The Epley maneuver or repositioning maneuver is a maneuver used to treat benign paroxysmal positional vertigo of the posterior or anterior canals

Robotic-assisted endoscopic thyroid surgery using the daVinci® Surgical System can safely and effectively offer those needing thyroid surgery relief without neck incisions. Dr. Ron Kuppersmith and Dr. Andrew deJong are now performing this procedure at the College Station Medical Center in Texas.

Implant comparison: Coloplast vs AMS for Penile Implants

Vetical Mattress Suture

Panic attack from Injection:'(

Interlocking Continuous Suture
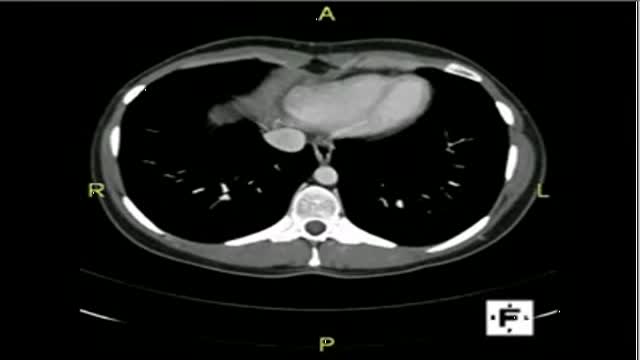
The video will describe anatomical structures as seen on a CT scan. Please see discalimer on my website.

This video: Blisters caused by friction or minor burns do not require a doctor's care. New skin will form underneath the affected area and the fluid is simply absorbed. Do not puncture a blister unless it is large, painful, or likely to be further irritated. The fluid-filled blister keeps the underlying skin clean, which prevents infection and promotes healing.

This baby was born with an adult sized tongue - and she just completed a surgery that will change her life.
http://eliminar-seu-diabetes.good-info.co/ Tipos De Diabetes, Diabets, Alimentação Para Diabéticos, Diabetes Tipo Ii, Yacon Diabetes, https://youtu.be/iDK8jKuR_VQ É provável que se sinta identificado com alguma destas situações. Tem medo de uma complicação a longo prazo, como a perda da visão, a amputação dos dedos dos pés, de extremidades ou inclusive da morte? Quer terminar com as injeções diárias de insulina e as picadas nos dedos? Enfrenta diariamente o fato de que tem 80% de probabilidades de morrer com doenças cardíacas ou derrame cerebral? Sofre de excesso de peso que não pode eliminar, causada por seus medicamentos? Quer deixar de se sentir culpado por ter dietas especiais que complicam a organização da sua família? Está oprimido pelo cuidado e controle que diariamente esta doença precisa? Quer deixar de sofrer os terríveis efeitos secundários que provocam os medicamentos para o Diabetes? Sei o que se sente. pensar que não existe esperança, que não tem cura e que estamos condenados a viver doentes. Mas hoje Tenho Excelentes Notícias para lhe dar e posso garantir que o que você vai ler neste site será o mais importante que tenha lido em toda a sua vida.
top 10 most incredible surgeries ever done

Cognitive impairment is seen in over half of people with multiple sclerosis. In this video I review factors that can contribute to multiple sclerosis brain fog, ways to assess cognition, and tips to improve thinking and memory.

Powerful results. Lasting effects. Medical approach. Rejuvenation therapy. Hormone treatments. Skin improvement. Revitalizing care. https://health4lifed.blogspot.com/

Superior vena cava syndrome (SVCS) is obstruction of blood flow through the superior vena cava (SVC). It is a medical emergency and most often manifests in patients with a malignant disease process within the thorax. A patient with SVCS requires immediate diagnostic evaluation and therapy.
A cornea transplant, also called keratoplasty, is a surgical procedure to replace part of your cornea with corneal tissue from a donor. Your cornea is the transparent, dome-shaped surface of your eye that accounts for a large part of your eye's focusing power. A cornea transplant can restore vision, reduce pain and improve the appearance of a damaged or diseased cornea. Most cornea transplant procedures are successful. But cornea transplant carries a small risk of complications, such as rejection of the donor cornea.

