- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

demonstrates how the Epley maneuver is performed to treat POSTERIOR canal BPPV affecting the right ear. Animation showing what is going on within the inner ear is also shown in the 2nd half of the video.

Vetical Mattress Suture

Interlocking Continuous Suture
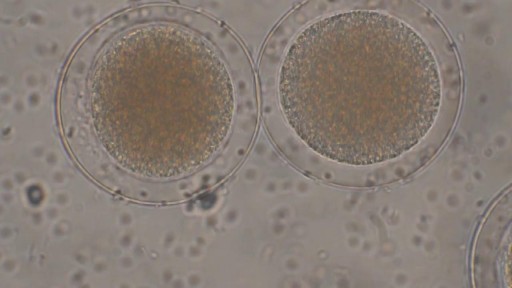
Sperm Meets Egg: Weeks 1 to 3 of Pregnancy. Something magical is about to happen! Watch as the ovulation process occurs, and then millions of sperm swim upstream on a quest to fertilize an egg. Your due date is calculated from the first day of your last menstrual period

Identify the anatomy and explain the physiology of the breast on diagrams and sonograms.
Describe and demonstrate the protocol for sonographic scanning of the breast, including the clock and quadrant methods, and targeted examinations based on mammographic findings.
Describe the various diagnostic pathways that may lead to a sonographic breast examination, and explain how the ultrasound findings are correlated with other imaging modalities.
Identify and describe sonographic images of benign and malignant features and common breast pathologies.
Explain biopsy techniques for breast tumors.
Define and use related medical terminology.
Explain the Patient Privacy Rule (HIPAA) and Patient Safety Act (see reference
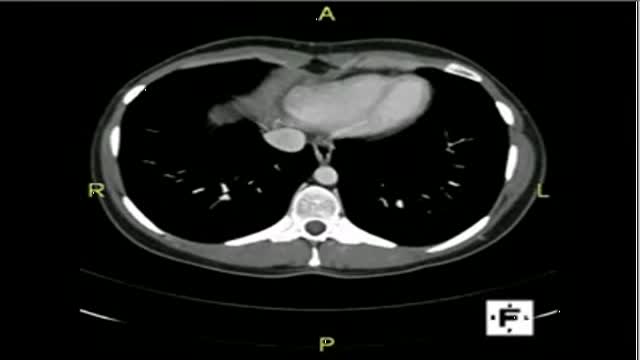
The video will describe anatomical structures as seen on a CT scan. Please see discalimer on my website.

Curious about physiotherapy or wanting to know how to properly perform an exercise? Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog
This video demonstrates how to perform a cardiovascular examination in an OSCE station.
You can access our step-by-step OSCE guide to accompany this video here: https://geekymedics.com/cardio....vascular-examination
Check out our other awesome clinical skills resources including:
• 🔥 Geeky Medics Bundles (discounted products): https://app.geekymedics.com/purchase/bundles/
• ✨ 1000+ OSCE Stations: https://app.geekymedics.com/pu....rchase/osce-stations
• 🏥 Geeky Medics OSCE Revision Book: https://app.geekymedics.com/purchase/book/
• 📝 150+ PDF OSCE Checklists: https://geekymedics.com/pdf-osce-checklists/
• 🗂️ 3000+ OSCE Flashcards: https://app.geekymedics.com/pu....rchase/flashcard-col
• 📱 Geeky Medics OSCE App: https://geekymedics.com/geeky-medics-app/
• 🩺 Medical Finals SBA Question Pack: https://app.geekymedics.com/pu....rchase/medical-stude
• 💊 PSA Question Pack: https://app.geekymedics.com/pu....rchase/prescribing-s
Chapters:
- Introduction 00:00
- General inspection 00:35
- Hands 00:46
- Schamroth's window test 01:07
- Capillary refill 01:27
- Pulses 01:35
- Carotid auscultation 02:21
- Carotid pulse 02:43
- Jugular venous pressure 02:55
- Hepatojugular reflux 03:09
- Inspection of the face 03:21
- Inspection of the chest 03:49
- Apex beat 04:12
- Heaves and thrills 04:28
- Heart valve ausculation 04:49
- Accentuation manoeuvres 05:45
- Lung base auscultation 06:23
- Sacral and pedal oedema 06:43
- Summary 07:10
Subscribe to our newsletter to be the first to know about our latest content: https://geekymedics.com/newsletter/ ✉️
Join the Geeky Medics community: 👩👩👧👧
Twitter: http://www.twitter.com/geekymedics
Instagram: https://instagram.com/geekymedics
Facebook: http://www.facebook.com/geekymedics
Always adhere to your medical school/local hospital guidelines when performing examinations or clinical procedures. DO NOT perform any examination or procedure on patients based purely upon the content of these videos. Geeky Medics accepts no liability for loss of any kind incurred as a result of reliance upon the information provided in this video.
Normal heart sounds and aortic regurgitation/stenosis sounds
Recorded on a Thinklabs Digital Stethoscope (https://www.thinklabs.com)
Some people have found this video useful for ASMR purposes.

Testosterone Booster, How To Get Testosterone, How To Improve Testosterone, Male Hormones
http://testosterone-booster.info-pro.co
Do This And Get Instantly Bigger Testicles
Today we're going to talk about the Stop And Go Method.
This tip is fun and easy to implement.
And your girl will absolutely love it Trust me on this
Here's the technique in a nutshell:
When doing the deed with your partner, take yourself just to the point of climax.
Then withdraw.
But don't just lay there while you wait for the peak to subside...
Kiss her, tease her, use your fingers, etc.
Watch this video and discover how to get much bigger testicles:
http://testosterone-booster.info-pro.co
Subscribe to our channel
http://natural-testosterone-boosters.blogspot.com/
https://www.youtube.com/watch?v=DPTeonpTBEM
Testosterone Booster, How To Get Testosterone, How To Improve Testosterone, Male Hormones,
how do you increase girth,
testosterone natural supplements,
improving sperm motility,
testosterone booster reviews,
girth increase,
how to increase my testosterone,
otc natural testosterone replacement,
testosterone increase,
are there foods that increase testosterone,
testosterona,
testosterone injections,
increasing testosterone naturally,
treatment for low testosterone,

In this video, I have covered Inguinal hernia under the following headings: Definition, Parts of Hernia, Surgical anatomy, Types of inguinal hernia, Aetiology of hernia, Clinical features of hernia, complications of hernia, Clinical examination, Surgical principles, and explanation of a few surgeries (Herniotomy, Bassini suture repair, Shouldice repair, Lichtenstein tension-free open meshplasty, hernia plugs, Laparoscopic techniques like TEP(Totally extraperitoneal approach) and TAPP(Transabdominal preperitoneal approach) surgical procedures).
SUBSCRIBE FOR MORE VIDEOS!
How to study General Surgery in med school: (Tips and Tricks)
https://youtu.be/_tad4i2Kdes
1-minute hernia videos: (Complete playlist by Skeleton)
https://www.youtube.com/watch?v=GsmAPYMiK_s&list=PL-dMZTUxuTxAi7rFqOy9o0pv1g-aZ1GXz
(includes femoral hernia, obturator hernia, epigastric hernia, umbilical hernia, Spigelian hernia, Richter hernia, lumbar hernia, incisional hernia, Hiatal hernia, congenital diaphragmatic hernia, contents of spermatic cord, triangles of hernia)
Study with me:
https://www.youtube.com/watch?v=lBkmmYcUBDo&t=291s
Hydrocele video:
https://www.youtube.com/watch?v=s6ICxMMtpYk&t=65s
You can support my channel by buying me a coffee here:
https://www.buymeacoffee.com/medvids
(Lecture slides will be available in the "EXTRAS" section of this link)
Instagram: @medvidsmadesimple
Check out my other works: linktr.ee/doctorcool
Testosterone treatment in adolescent boys with constitutional delay

Computed tomography (CT)-guided transthoracic needle biopsy is a well-established, minimally invasive diagnostic tool for pulmonary lesions. Few large studies have been conducted on the diagnostic performance and adequacy for molecular testing of transthoracic core needle biopsy (TCNB) for small pulmonary lesions.

This video: Blisters caused by friction or minor burns do not require a doctor's care. New skin will form underneath the affected area and the fluid is simply absorbed. Do not puncture a blister unless it is large, painful, or likely to be further irritated. The fluid-filled blister keeps the underlying skin clean, which prevents infection and promotes healing.

Our General Surgery team treats hernia patients on a daily basis. In fact, you could consider them to be hernia experts. We sat down with one of those experts, Dr. Heater Dunlap, to talk about the common signs and symptoms of hernias and to answer the question of when to see a doctor.
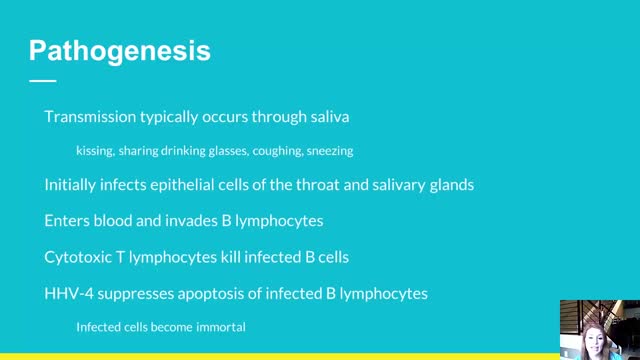
This patient has infectious mononucleosis (IM), a disease caused by the Epstein-Barr virus. IM is a systemic viral infection that is usually seen in children and adolescents. The common presentation is fever with pharyngitis or tonsillitis, cervical adenopathy, splenomegaly, and mild hepatitis.
Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia. Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.

To avoid pregnancy and STDs, always remember to use a condom every time you have sex — including oral, vaginal, or anal sex. Whenever oral sex is being performed on a girl, a dental dam should be used. A guy receiving oral sex should wear a latex condom — or, if he or his partner is allergic to latex, a polyurethane condom.

We will show how to know if you have a sports hernia. These are a few tests you can do on your own. Lower abdominal pain and tightness that increases with twisting and kicking. Stretching and exercises tend to make the discomfort increase.
Want more info? We have a free webinar that covers hip, groin, adductor, lower abdominal strains and sports hernia diagnosis in detail. Use this link to get access. https://bit.ly/37thtNF
#sportshernia #hernia #hippain
To work with us, contact us using this link https://bit.ly/3zCBnzZ or call us 714-502-4243. We have online programs, virtual and in-person options.
Costa Mesa, CA www.p2sportscare.com
Option 1: Groin On-Demand Webinar https://bit.ly/37thtNF
Option 2: Video Guide https://bit.ly/33aLIqC
Option 3 (the best): Work With Us https://www.p2sportscare.com/
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
http://eliminar-seu-diabetes.good-info.co/ Tipos De Diabetes, Diabets, Alimentação Para Diabéticos, Diabetes Tipo Ii, Yacon Diabetes, https://youtu.be/iDK8jKuR_VQ É provável que se sinta identificado com alguma destas situações. Tem medo de uma complicação a longo prazo, como a perda da visão, a amputação dos dedos dos pés, de extremidades ou inclusive da morte? Quer terminar com as injeções diárias de insulina e as picadas nos dedos? Enfrenta diariamente o fato de que tem 80% de probabilidades de morrer com doenças cardíacas ou derrame cerebral? Sofre de excesso de peso que não pode eliminar, causada por seus medicamentos? Quer deixar de se sentir culpado por ter dietas especiais que complicam a organização da sua família? Está oprimido pelo cuidado e controle que diariamente esta doença precisa? Quer deixar de sofrer os terríveis efeitos secundários que provocam os medicamentos para o Diabetes? Sei o que se sente. pensar que não existe esperança, que não tem cura e que estamos condenados a viver doentes. Mas hoje Tenho Excelentes Notícias para lhe dar e posso garantir que o que você vai ler neste site será o mais importante que tenha lido em toda a sua vida.

Amazing Lung Inflation
