- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Vaginal Hysterectomy Procedure of a 42 years old female patient with a 3 months history of symptomatic vaginal bulge
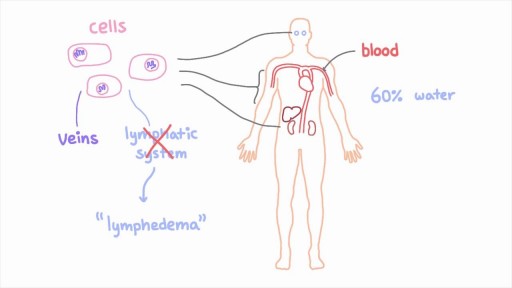
The lymphatic system is a network of specialized vessels (lymph vessels) throughout the body whose purpose is to collect excess lymph fluid with proteins, lipids, and waste products from the tissues. This fluid is then carried to the lymph nodes, which filter waste products and contain infection-fighting cells called lymphocytes. The excess fluid in the lymph vessels is eventually returned to the bloodstream. When the lymph vessels are blocked or unable to carry lymph fluid away from the tissues, localized swelling (lymphedema) is the result.
This video is designed for my introductory A&P course to study the endocrine system. This tutorial will take you through the various endocrine organs, hormones produced, and effects at each tissue. Prolactin is one of the 5 hormones we are studying of the anterior pituitary. SHOW MORE
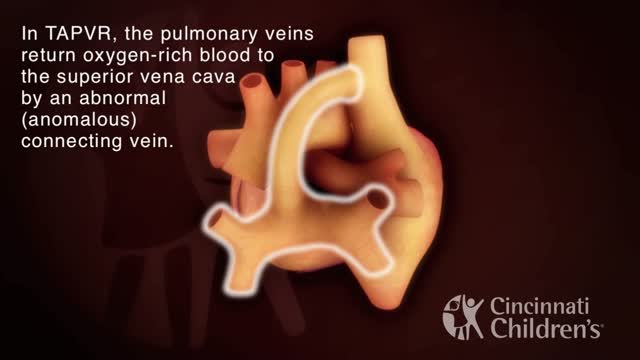
Total anomalous pulmonary venous return (TAPVR) is a rare congenital malformation in which pulmonary veins that return oxygen-rich blood from the lungs do not connect normally to the left atrium. Instead all four pulmonary veins drain abnormally to the right atrium. Heart models and animation were developed by the Cincinnati Children's Heart Institute in conjunction with Cincinnati Children's Critical Care Media Lab.
Learn what's working for other Nursing Students! Check out our Top 10 Most Popular Lessons Here: https://bit.ly/3nda5u3
Get the full lesson here: https://nursing.com/lesson/ski....lls-03-04-trach-care
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
Trach Care Overview (Nursing Skills):
In this video we’re going to look at trach care. Remember you should always suction the patient before trach care, so if you haven’t watched that skill video yet, make sure you watch it!
Click here: https://nursing.com/lesson/ski....lls-03-03-trach-suct
And remember as you’re doing this, you want to be assessing the stoma for signs of infection or skin breakdown.
Bookmarks:
0:00 Introduction
0:30 Set up sterile field
1:00 Apply gloves
1:12 Remove inner canula and dressing
1:30 Apply sterile gloves
2:05 Clean secretions
2:56 Clean stoma
3:48 Replace inner canula
4:14 Change trach ties
5:50 Apply dressing
Visit us at https://nursing.com/medical-disclaimer/ for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

To avoid pregnancy and STDs, always remember to use a condom every time you have sex — including oral, vaginal, or anal sex. Whenever oral sex is being performed on a girl, a dental dam should be used. A guy receiving oral sex should wear a latex condom — or, if he or his partner is allergic to latex, a polyurethane condom.
A video showing how to deal with electrical burns and their first aid

A subdural hematoma is most often the result of a severe head injury. This type of subdural hematoma is among the deadliest of all head injuries. The bleeding fills the brain area very rapidly, compressing brain tissue. This often results in brain injury and may lead to death. Subdural hematomas can also occur after a minor head injury. The amount of bleeding is smaller and occurs more slowly. This type of subdural hematoma is often seen in older adults. These may go unnoticed for many days to weeks, and are called chronic subdural hematomas. With any subdural hematoma, tiny veins between the surface of the brain and its outer covering (the dura) stretch and tear, allowing blood to collect. In older adults, the veins are often already stretched because of brain shrinkage (atrophy) and are more easily injured.

A biopsy is a diagnostic test that involves collecting small pieces of tissue, usually through a needle, for examination with a microscope. A kidney biopsy can help in forming a diagnosis and in choosing the best course of treatment.

Hernia symptoms test diagnosis and surgery - This lecture explains about hernia symptoms, diagnosis and surgery to cure hernia disease. Stay tuned to this video lecture to get answer of the following questions -
what is hernia disease?
hernia symptoms?
hernia test?
hernia diagnosis?
hernia treatment?
Specifically the hernia surgery is explained in this video. So stay tuned to this video to more about hernia repair and details about hernia symptoms and diagnosis.
Watch this video lecture if you have hernia and want to know about hernia surgery and hernia operation related information.
For more information, log on to-
http://[a]www.shomusbiology.com%2F[/a]
Get Shomu's Biology DVD set here-
http://[a]www.shomusbiology.com%2F[/a]dvd-store/
Download the study materials here-
http://shomusbiology.com/bio-materials.html
Remember Shomu’s Biology is created to spread the knowledge of life science and biology by sharing all this free biology lectures video and animation presented by Suman Bhattacharjee in YouTube. All these tutorials are brought to you for free. Please subscribe to our channel so that we can grow together. You can check for any of the following services from Shomu’s Biology-
Buy Shomu’s Biology lecture DVD set- [a]www.shomusbiology.com%2Fdvd-store[/a]
Shomu’s Biology assignment services – [a]www.shomusbiology.com%2Fassignment[/a] -help
Join Online coaching for CSIR NET exam – [a]www.shomusbiology.com%2Fnet-coaching[/a]
We are social. Find us on different sites here-
Our Website – www.shomusbiology.com
Facebook page- https://www.facebook.com/ShomusBiology/
Twitter - https://twitter.com/shomusbiology
SlideShare- www.slideshare.net/shomusbiology
Google plus- https://plus.google.com/113648584982732129198
LinkedIn - https://www.linkedin.com/in/su....man-bhattacharjee-2a
Youtube- https://www.youtube.com/user/TheFunsuman
Thank you for watching the health tutorial video on Hernia symptoms test diagnosis and surgery.
The hepatitis E virus, responsible for major epidemics of viral hepatitis in subtropical and tropical countries, was cloned only 7 years ago.1 Hepatitis E was found to belong to the family of Caliciviridae, which includes the Norwalk virus—a common cause of gastroenteritis in humans—and consists of a single, plus-strand RNA genome of approximately 7.2 kb without an envelope (Fig. 1). The virus contains at least three open reading frames encoding viral proteins against which antibodies are made on exposure. These antibodies, especially those against the capsid protein derived from the second open reading frame2 and a protein of unknown function derived from the third open reading frame, are detected by currently available serologic assays. Retrospective studies on stored sera of past epidemics of viral hepatitis in Mexico, Africa, Afghanistan, Pakistan, India, Bangladesh, Burma, Nepal, and Borneo have revealed that all were caused by strains of hepatitis E. In addition, hepatitis E was found to be responsible for the hepatitis epidemic in the southern part of Xinjiang, China, in which 120,000 persons became infected between September 1986 and April 1988.3 Hepatitis E predominantly affects young adults (15 to 40 years old). The symptoms of hepatitis E are similar to those of hepatitis A. Frequently, a prodrome consisting of anorexia, nausea, low-grade fever, and right upper abdominal pain is present 3 to 7 days before jaundice develops. Aminotransferase levels peak (usually between 1,000 and 2,000 U/L) near the onset of symptoms; bilirubin levels (10 to 20 mg/dL) peak later. Jaundice usually resolves after 1 to 2 weeks. In about 10% of cases, the disease is fulminant—especially in pregnant women, among whom mortality rates as high as 20% due to hemorrhagic and thrombotic complications have been reported. No evidence has suggested that hepatitis E can cause chronic infection. Transmission is by the fecal-oral route, predominantly through fecally contaminated drinking water supplies. In addition, however, preliminary reports have suggested transmission of the hepatitis E virus through blood transfusions. Volunteer studies confirmed the presence of the virus in serum and feces before and during clinical disease.4 The virus is shed into feces approximately 1 week before symptoms develop. The incubation period varies from 2 to 9 weeks (mean duration, approximately 45 days). Until now, a few reports had described symptomatic hepatitis E acquired in Europe;5, 6 all patients with symptomatic hepatitis E in the United States were travelers returning from Mexico, Africa, or the Far East, in whom hepatitis E developed after their return home.7 In this issue of the Mayo Clinic Proceedings (pages 1133 to 1136), Kwo and associates describe a case of hepatitis E in a man who had not left the United States during the previous 10 years. Specific serologic tests for hepatitis E virus IgG (enzyme immunoassays and a fluorescent antibody blocking assay) and IgM8 (US strain-specific enzyme-linked immunosorbent assay with use of synthetic polypeptides deduced from the viral genome, as shown in Figure 1), developed at Abbott Laboratories (IgG and IgM) as well as at the Centers for Disease Control and Prevention (IgG), were used to prove that the patient indeed had acute hepatitis E. Researchers at Abbott Laboratories have prepared a report that describes most of the viral genome in this patient (Fig. I).8 Their results are interesting because this strain from the United States differs considerably from hepatitis E strains isolated in Mexico, Burma, Pakistan, or China. Furthermore, the sequence of the US strain is highly homologous (98% and 94% homology at the amino acid level to the second and third open reading frames, respectively) to a recently isolated hepatitis E strain from American swine.9 This finding suggests that, in the United States, hepatitis E is a zoonosis with the swine population as one of its hosts. This relationship would confirm earlier studies in Asia, where swine were also found to carry variants of the hepatitis E virus.10 Why are these two recent discoveries important for medicine in the United States? First, other sporadic, locally acquired cases of acute hepatitis may be caused by hepatitis E. Second, these back-to-back discoveries strongly suggest that a common natural host for hepatitis E is present in countries with more moderate climates. Because swine do not seem to experience any symptoms associated with infection and because symptoms in humans can be minor or absent, we now may also have an explanation for the 1 to 2% of positive hepatitis E serologic results in blood donors in the United States,11 Netherlands,12 and Italy,6 countries with large swine staples. Clearly, more research needs to be done to confirm this hypothesis. Third, in countries with more moderate climates, hepatitis E may often result in a subclinical infection. Is this variation in manifestation due to less virulent strains, and do sequence variations determine virulence? Fourth, swine may be used as an animal model for study of the disease as well as vaccine development.

Our surgeons take a compassionate, family-centered approach to both inpatient and outpatient care. We’re committed to making sure both you and your child understand our process. Told through a kid's eyes, this video tour reveals our caring approach.
To learn more about pediatric surgery at Stamford Hospital, visit: https://www.stamfordhealth.org..../care-treatment/pedi

Delorme Operation for Rectal Prolapse

Avideo showing suturing of the uterus and abdominal wall after c-section

When your child needs surgery, it can be overwhelming and sometimes scary. At Mayo Clinic Children’s Center, our highly skilled surgeons apply deep experience and specialized training to offer individualized care for your child and your family.

In vitro fertilization, or IVF, is the most common and effective type of assisted reproductive technology to help women become pregnant. It involves fertilizing an egg outside the body, in a laboratory dish, and then implanting it in a woman's uterus. By 2016, some 6.5 million babies had been born using in-vitro fertilization (IVF). According to the Centers for Disease Control and Prevention (CDC), around 1.6 percent of babies born in the United States each year are conceived through assisted reproductive technology (ART).
Ejaculating into a partner’s mouth is a common practice during oral sex/fellatio. In a safe situation (where there is no danger of catching an STD), the semen-receiving partner may choose to spit the semen out, or to swallow it. Before you engage in fellatio, I’d recommend that you and your partner both get tested for sexually transmitted infections (STIs). If not, please use barriers for oral sex and abstaining from making contact with ejaculate. Semen is mostly water, but also contains amino acids and protein, sugars such as fructose and glucose, minerals such as zinc and calcium, vitamin C, and a few other nutrients. Sperm cells themselves make up less than one percent of semen. Semen is edible, and if swallowed, will travel down the esophagus and into the stomach, where it will be digested in the same way that food is. You can never get pregnant by swallowing semen. Some people accept the taste of semen, but others complain that swallowing semen can give them an upset stomach. In rare cases, you may have an allergy to the proteins found in semen. What does It Taste Like? The taste of semen varies. Bitter, sweet, metallic. So, one may expect to find the taste of semen anywhere from enjoyable to tasteless to disgusting. But there is a way of controlling the taste of semen, which is through diet. Keep track of the diet, and communicate with the partner about when it tastes better or worse.

Histology of Neurovascular Bundle

http://without-glasses.good-info.co How To Improve Eyesight Naturally With Food , How To Improve Eyesight Naturally With Exercises Food. Naturally PERFECT your Vision to 20/20 If you are one of the millions of Americans who suffer from visual problems such as Myopia and Hyperopia then this video will SHOCK you! In the following free video you'll discover: How you can 100% naturally and safely cure almost any visual problem. Why your glasses and contacts are in fact WORSENING your eye condition. The real TRUTH about the Eyecare industry This revolutionary program that you'll soon discover has dared to challenge the billion-dollar Eyecare industry. It reveals this amazing secret to getting 20/20 vision and it doesn't matter what your eye problems are, whether short or long sightedness, Presbyopia, Glaucoma.. whatever! It should help with everything. more information in. http://without-glasses.good-info.co
Myth About Night Fall (Nocturnal Ejaculation) ۔ احتلام کوئی بیماری نہیں۔ 3
