- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
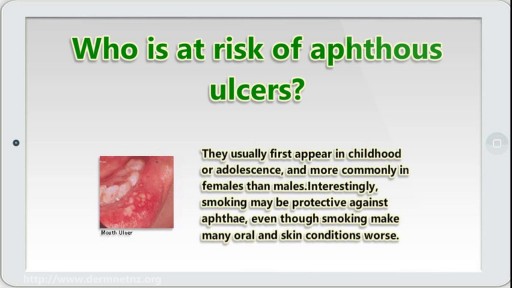
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Interlocking Continuous Suture
Testosterone treatment in adolescent boys with constitutional delay
Symptoms of liver failure include vomiting, diarrhea and fatigue as well as the symptoms from stage 3. While the progression from cirrhosis to failure can take years, the damage is irreversible and leads to eventual death. The key to treating liver disease is to diagnose the condition as early as possible.

Toilet Training Boys, Training Potty, Best Way To Potty Train, What Age Do You Potty Train
http://potty-training-fast.good-info.co
Wanna have some fun imagining life without diapers?
Imagine if your child would disappear on their own
one minute and all of a sudden the next minute you
hear the toilet flush and the sink start to run.
Can you imagine it?
Life becomes so much easier the second your child
becomes potty trained and you start to wonder why
you didn't just get it over with sooner...
Would you start potty training right this weekend
if I handed you a guide that guaranteed to get your
child out of diapers in just 3 days?
Click the link below to check it out
http://potty-training-fast.good-info.co
Subscribe to our channel
http://potty-training-fast.blogspot.com/
https://www.youtube.com/watch?v=ck-4RTvP5F4
Toilet Training Boys, Training Potty, Best Way To Potty Train, What Age Do You Potty Train,
3day potty training,
toilet training tips for girls,
how to do potty training,
best potty training book,
potty training boys the easy way,
potty training activities,
how to potty training,
potty training video for toddlers,
when do you potty train,
how to potty train a kid,
potty training at 18 months,
havanese potty training,
how to potty train your baby,

The Epley maneuver or repositioning maneuver is a maneuver used to treat benign paroxysmal positional vertigo of the posterior or anterior canals
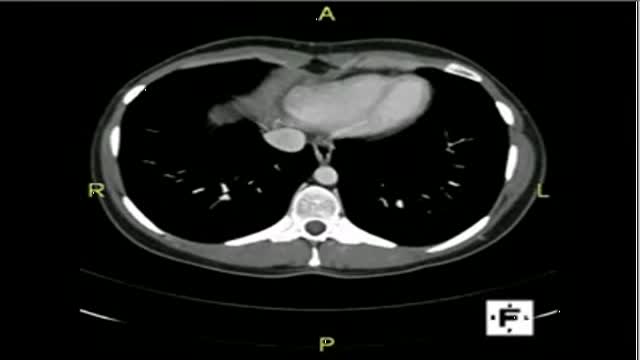
The video will describe anatomical structures as seen on a CT scan. Please see discalimer on my website.
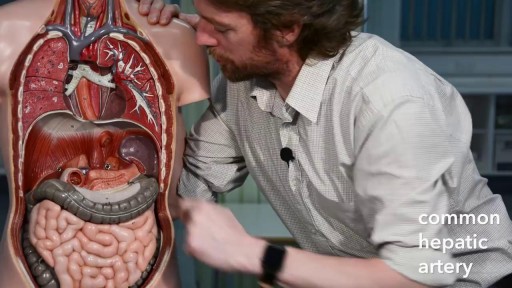
The primary functions of the liver are: Bile production and excretion. Excretion of bilirubin, cholesterol, hormones, and drugs. Metabolism of fats, proteins, and carbohydrates. Enzyme activation. Storage of glycogen, vitamins, and minerals. Synthesis of plasma proteins, such as albumin, and clotting factors.

demonstrates how the Epley maneuver is performed to treat POSTERIOR canal BPPV affecting the right ear. Animation showing what is going on within the inner ear is also shown in the 2nd half of the video.
This patient has infectious mononucleosis (IM), a disease caused by the Epstein-Barr virus. IM is a systemic viral infection that is usually seen in children and adolescents. The common presentation is fever with pharyngitis or tonsillitis, cervical adenopathy, splenomegaly, and mild hepatitis.

SUBSCRIBE: https://www.youtube.com/c/TVNe....phrologist?sub_confi
An animation of blood flow inside the Hemodialysis circuit.
About Dr. Rifai:
Dr. Ahmad Oussama Rifai is certified by the American Board of Internal Medicine (ABIM) in the specialty of Internal Medicine and the sub-specialty of Nephrology.
MEET DR. RIFAI
https://www.thevirtualnephrologist.com/rifai/
Follow The Virtual Nephrologist on SOCIAL MEDIA:
-Facebook: https://www.facebook.com/thevirtualnephrologist
-Instagram: https://www.instagram.com/thevirtualnephrologist/
-Twitter: https://twitter.com/VNephrologist
Schedule a virtual consult:
https://www.thevirtualnephrolo....gist.com/schedule-a-
Best wishes for great health | The Virtual Nephrologist
Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia. Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.

The OrthoIllustrated® animation for total knee replacement is an educational tool to help patients better understand the diagnosis and treatment of arthritis.
- - - - -
Why Work Arthrex https://www.arthrex.com/job-seeker
Find an Arthrex Surgeon: https://doctorfinder.orthoillustrated.com
- - - - -
Join the Community:
LinkedIn: https://www.linkedin.com/company/arthrex
Facebook: https://www.facebook.com/Arthrex
Instagram: https://www.instagram.com/arthrex_inc/
Twitter: https://twitter.com/Arthrex
TikTok: https://www.tiktok.com/@arthrex
- - - - -
Arthrex Inc., headquartered in Naples, Florida, is a global leader in orthopedic surgical device design, research, manufacturing, and medical education. Arthrex develops and releases more than 1,000 new products and procedures every year to advance minimally invasive orthopedics worldwide.
For more information, visit https://www.arthrex.com
- - - - -
OrthoPedia is an innovative educational website that was created for anyone interested in learning about orthopedics from the first-year student to the experienced orthopedic surgeon.
Visit https://www.orthopedia.com to experience the future of Medical Education.

Cerclage is indicated in a patient with a history of painless cervical dilation and a second trimester loss. It is also indicated in a patient with a history of preterm birth and a short cervix found on ultrasound between 16-24 weeks gestation. Cerclage placement occurs after the first trimester in case the pregnancy is genetically abnormal and would likely result in a first trimester loss.

AL EMADI HOSPITAL-QATAR-DOHA
AMERICAN BOARD CERTIFICATE AESTHETIC MEDICINE
0097455742973

In this video, I have covered Inguinal hernia under the following headings: Definition, Parts of Hernia, Surgical anatomy, Types of inguinal hernia, Aetiology of hernia, Clinical features of hernia, complications of hernia, Clinical examination, Surgical principles, and explanation of a few surgeries (Herniotomy, Bassini suture repair, Shouldice repair, Lichtenstein tension-free open meshplasty, hernia plugs, Laparoscopic techniques like TEP(Totally extraperitoneal approach) and TAPP(Transabdominal preperitoneal approach) surgical procedures).
SUBSCRIBE FOR MORE VIDEOS!
How to study General Surgery in med school: (Tips and Tricks)
https://youtu.be/_tad4i2Kdes
1-minute hernia videos: (Complete playlist by Skeleton)
https://www.youtube.com/watch?v=GsmAPYMiK_s&list=PL-dMZTUxuTxAi7rFqOy9o0pv1g-aZ1GXz
(includes femoral hernia, obturator hernia, epigastric hernia, umbilical hernia, Spigelian hernia, Richter hernia, lumbar hernia, incisional hernia, Hiatal hernia, congenital diaphragmatic hernia, contents of spermatic cord, triangles of hernia)
Study with me:
https://www.youtube.com/watch?v=lBkmmYcUBDo&t=291s
Hydrocele video:
https://www.youtube.com/watch?v=s6ICxMMtpYk&t=65s
You can support my channel by buying me a coffee here:
https://www.buymeacoffee.com/medvids
(Lecture slides will be available in the "EXTRAS" section of this link)
Instagram: @medvidsmadesimple
Check out my other works: linktr.ee/doctorcool

Benzodiazepines are a class of agents that work on the central nervous system, acting selectively on gamma-aminobutyric acid-A (GABA-A) receptors in the brain. GABA is a neurotransmitter that inhibits or reduces the activity of nerve cells (neurons) within the brain. Benzodiazepines open GABA-activated chloride channels, and allow chloride ions to enter the neuron. This makes the neuron negatively charged and resistant to excitation.

Powerful results. Lasting effects. Medical approach. Rejuvenation therapy. Hormone treatments. Skin improvement. Revitalizing care. https://health4lifed.blogspot.com/

Eating a high-protein breakfast has been shown to reduce cravings and calorie intake throughout the day (16, 17). Avoid sugary drinks and fruit juice. These are the most fattening things you can put into your body, and avoiding them can help you lose weight (18, 19). Drink water a half hour before meals.
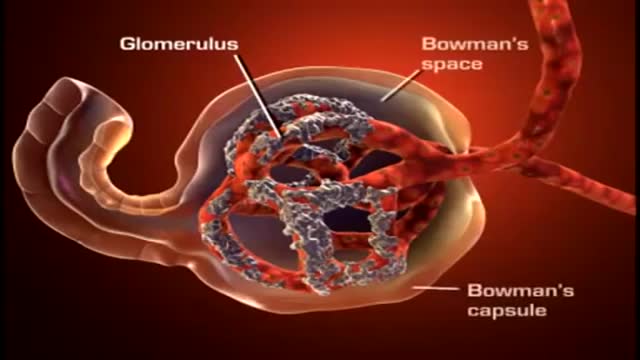
A nephron (from Greek νεφρός (nephros) meaning "kidney") is the basic structural and functional unit of the kidney. Its chief function is to regulate the concentration of water and soluble substances like sodium salts by filtering the blood, reabsorbing what is needed and excreting the rest as urine.