- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which carries sensation from your face to your brain. If you have trigeminal neuralgia, even mild stimulation of your face — such as from brushing your teeth or putting on makeup — may trigger a jolt of excruciating pain. You may initially experience short, mild attacks. But trigeminal neuralgia can progress and cause longer, more-frequent bouts of searing pain. Trigeminal neuralgia affects women more often than men, and it's more likely to occur in people who are older than 50. Because of the variety of treatment options available, having trigeminal neuralgia doesn't necessarily mean you're doomed to a life of pain. Doctors usually can effectively manage trigeminal neuralgia with medications, injections or surgery.

Follow along on a typical day with UCSF Medical Center's chief of cardiothoracic surgery Dr. Tom Nguyen. Take a walk on rounds with his team as they check on patients who are recovering or preparing for heart valve surgeries to treat conditions such as mitral valve prolapse and mitral regurgitation. Get a glimpse into the operating room as Dr. Nguyen and his team use the latest non-invasive techniques to help patients achieve the best outcomes.
0:00 Surgeon begins day with morning report
0:53 Meet with fellows and visit patients
1:28 Surgeon thoughts on his practice
Minimally Invasive Surgeries
2:09 Mitral valve replacement for mitral stenosis
3:11 Mitral valve repair for AFib and mitral regurgitation
3:36 Stopping the heart
4:15 Culture 1 - Everyone's voice matters
4:45 Mitral valve repair for heart murmur
5:12 Culture 2 - Patient first
To view more UCSF videos relating to Mitral Regurgitation Treatment and Aortic Stenosis Treatment view:
Mitral Regurgitation Treatment Options https://youtu.be/7nUUOMx4tJ0
Aortic Stenosis Treatment Options https://youtu.be/A2rZK0oFWcc
If you want to learn more about the Cardiac Surgery clinic and to request an appointment visit: https://www.ucsfhealth.org/cli....nics/cardiac-surgery
#dayinthelife #heartsurgeon #heartsurgery #CardiacSurgery #Cardiology #ucsf #drnguyen#ucsfhealth #Cardiothoracic

The video is about the evolution of the anatomic UCLA laparoscopic technique over 1325 cases and demonstrates the key steps of our operation to improve patient safety and outcomes.
Learn more at http://urology.ucla.edu

A thyroid biopsy is a procedure in which a small sample of tissue is removed from the thyroid gland and looked at under a microscope for cancer, infection, or other thyroid problems. The thyroid gland is found in front of the windpipe (trachea), just below the voice box (larynx). A sample of thyroid tissue can be taken by: Fine-needle biopsy. Your doctor puts a thin needle through the skin and into the thyroid gland. Many thyroid specialists like to use a needle biopsy method rather than surgery. Open biopsy. Your doctor makes a cut (incision) through the skin to see the thyroid gland. This method is done when other tests have not found the cause of your symptoms. Core needle biopsy. Your doctor inserts a needle with a special tip and removes a sample of tissue about the size of a grain of rice.

Totally Stapled Bowel Resection and Anastomosis

Facial Skin Cancer Surgery

LIS Closed done at 5 O clock position, using Scalpel blade 15. After feeling the groove between internal and external anal sphincter, the blade is passed in and the lower 1/2 of Internal anal sphincter is cut. Remain below dentate line. If anal mucosa is accidently cut suture with 4-0 rapid vicryl. In event of bleeding, pinchcock for 5 minutes.


Thoracic Epidural Placement Paramedian Approach

Carpal tunnel release (part 1). Skin incision and retraction. Procedure performed by Deepak Kapila, MD, Broward Health, Fort Lauderdale, FL. Courtesy of BroadcastMed (http://ortho.broadcastmed.com/....4229/videos/carpal-t
There are hundreds more procedural videos as well as news, features, resources and references on Medscape.com. Join today for free.

ormal sperm densities range from 15 million to greater than 200 million sperm per milliliter of semen. You are considered to have a low sperm count if you have fewer than 15 million sperm per milliliter or less than 39 million sperm total per ejaculate.
This video shows submandibular gland being surgically removed.

Endoscopic fenestration of suprasellar cyst in a 4 years old girl

Arterial line placement is a common procedure in various critical care settings. Intra-arterial blood pressure (BP) measurement is more accurate than measurement of BP by noninvasive means, especially in the critically ill. [1] Intra-arterial BP management permits the rapid recognition of BP changes that is vital for patients on continuous infusions of vasoactive drugs. Arterial cannulation also allows repeated arterial blood gas samples to be drawn without injury to the patient.
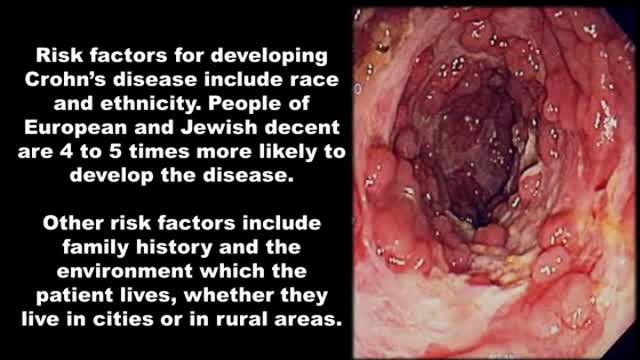
http://crohnsulcerativecolitis.plus101.com/
----Crohn's Disease Symptoms Pain. Are you suffering from diarrhea that sometimes leaves you feeling that you've completely emptied your intestine from eveything you've eaten that week?
Have you seen bright red blood traces in your stool or on the toilet paper at least once?
Do you sometimes have abdominal cramps after your meals?
Do you at times feel so nauseous that food doesn't have any appeal to you?
Have you had at least one onset of unexplained low grade fever?
Do you joints sometimes feel itchy, sore or painful?
Did you ever notice red spots or blisters on your arms or legs?
Did you ever experience episodes of itchy and even painfull pink eye (conjuctivitis)?
Have you lost weight?
Do you have episodes of overwhelming fatigue?
Do you experience increased frequency of bowel movement?
Did you ever get up during the night to defecate?
Crohn's, Disease, Symptoms, Pain, symptoms of crohns, chrons disease symptoms , ulcerative colitis symptoms, symptoms of colitis, United States, United Kingdom, Canada, ulcerative colitis diet, ulcerative colitis treatment, irritable bowel symptoms

Intussuseption and Appendectomy

Dr.Young Cho explains what happens during a tummy tuck procedure, and what he does to get that hourglass shape.
