- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Successful External Cephalic Version (ECV) - Turning a breech baby in just 2 minutes!

A spontaneous vaginal delivery (SVD) occurs when a pregnant woman goes into labor with or without use of drugs or techniques to induce labor, and delivers her baby in the normal manner, without forceps, vacuum extraction, or a cesarean section. Assisted vaginal delivery (AVD) occurs when a pregnant woman goes into labor with or without the use of drugs or techniques to induce labor, and requires the use of special instruments such as forceps or a vacuum extractor to deliver her baby vaginally.

Pinch air out of the tip of the condom. Unroll condom all the way down the penis. After sex but before pulling out, hold the condom at the base. Then pull out, while holding the condom in place. Carefully remove the condom and throw it in the trash.
Aspirin is a salicylate (sa-LIS-il-ate). It works by reducing substances in the body that cause pain, fever, and inflammation. Aspirin is used to treat pain, and reduce fever or inflammation. It is sometimes used to treat or prevent heart attacks, strokes, and chest pain (angina).

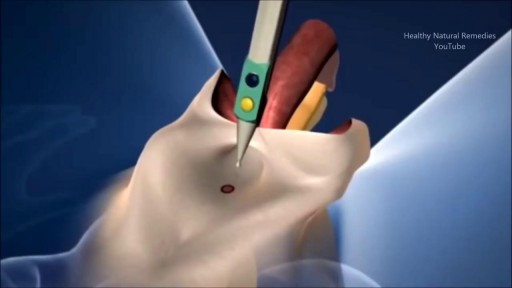
Surgical cutting and removal of a deep skin cyst Medical Videos
Ever wonder How Male to Female Trans'Gender Surgery works?

Direct Laryngoscopy: MICU Fellows Airway Course

ERROR

http://penilepapules.plus101.com/ ----- White Spots On Shaft, Pearly Penile Papules Treatment Cream, Single Red Bump On Shaft, Ppp Surgery. Common Home Made Remedies for Pearly Penile Papules. When it comes to treating pearly penile papules many people find it very difficult to reach one of the medical treatments. This is mainly because they are highly expensive and not many people can afford spending large amounts of money on surgery and recovery. In addition to that, these procedures have been reported as being quite risky, which make the men suffering from pearly penile papules think twice before going for one of the available surgeries. This is why, along the time, many homemade, natural treatments have been experienced, so that a cheaper and less risky way of curing pearly penile papules would be found. Some of the methods which have been tried proved to be very less effective, while some did not have any effect at all. Yet, there have also been methods which not only proved to be effective, but they were also considered to be much better than the medical treatment. Most of those who have tried the tea tree oil treatment reported significant diminish of the number of the papules from their penises. In addition to the clearing of the skin, they have also noticed that there were no side effects and the skin remained soft after the papules were removed. As the method was quite simple to put in practice (it requires the application of tea tree oil on the affected area with a cotton swab for three or four times per day), many men decided this was indeed a great solution to their problem.

Loyola Full Male Exam Part 3 A video from Loyola medical school, Chicago showing the full examination of the male

Surgeons at The Children’s Hospital of Philadelphia were the first to perform a bilateral hand transplant on a child. Our research and work in this groundbreaking field of medicine led us to establish the Hand Transplantation Program. Combining the expertise of the Penn Transplant Institute and the Hospital’s Division of Plastic and Reconstructive Surgery and Division of Orthopedics, the program aims to improve quality of life for children who may benefit from this procedure. This is Zion, one year after the surgery
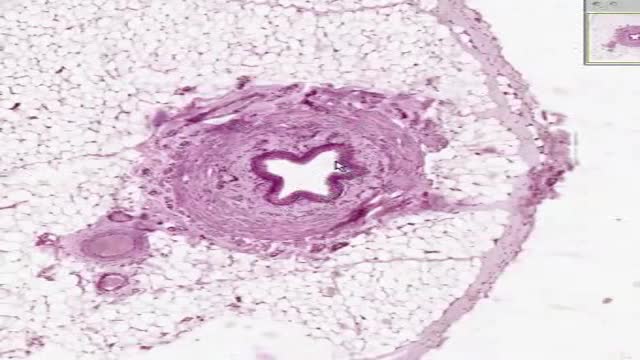
Histology of Ureter

Symptoms Of Anxiety, Anxiety Disorder Symptoms, What Is Social Anxiety, Zoloft For Anxiety --- http://panic-attacks-anxiety.good-info.co --- Panic attacks and anxiety While there are times for doctors, I want you to consider this: MOST of your anxiety is under the radar… Masquerading as “just feeling a bit nervous”... or “just a tad irritable thanks to this diet plan”... or, “let’s skip the party and just stay home tonight.” And, I’m telling you, that anxiety not only destroys your fat burning power: It often leads to all-out panic disorder, if you just ignore it. Fortunately for you, there’s a 60-Second Solution that restores your calm, removes those anxious feelings, and allows you to keep burning body fat for energy. Now, this exact same technique works for all-out panic and even more serious anxiety issues, too… The man who delivers this presentation had panic attacks in “everyday” situations… and he too had feelings of anxiety whenever he tried to diet-off body fat… This Simple Trick Stops Panic Attacks And Anxiety Click Here: http://panic-attacks-anxiety.good-info.co

http://plantar-fasciitis-solution.info-pro.co Foot Arch Pain, Sharp Pain In Heel, Pain In Foot, Achilles Heel Pain, Chronic Plantar Fasciitis What is Plantar Fasciitis? Plantar fasciitis is a common injury that affects the heel of a person’s foot. The arches of the feet are supported by a tough and fibrous tissue known as the plantar fascia and when this tissue is used repetitively, injury may occur. It can be easy to overuse the feet, especially when participating in activities such as sporting events. Hence, plantar fasciitis is more commonly found in athletes or others who are constantly using their feet for long durations. With excessive use, the planar fascia will eventually give in and this condition may also be progressive. Runners and those who are known to participate in similar activities need to ensure that they do not damage this important band of tissue. In addition, body weight could be a factor that leads to the occurrence of plantar fasciitis. If a person is overweight, the feet and subsequently the plantar fascia tissue could become overwhelmed. Improper footwear could also cause a strain on the plantar fascia tissue and this could gradually become severe over time. plantar fasciitis relief in 7 days click here. http://plantar-fasciitis-solution.info-pro.co

Draining a Hand Abscess

Urinary incontinence isn't a disease, it's a symptom. It can be caused by everyday habits, underlying medical conditions or physical problems. A thorough evaluation by your doctor can help determine what's behind your incontinence. Temporary urinary incontinence Certain drinks, foods and medications can act as diuretics — stimulating your bladder and increasing your volume of urine. They include: Alcohol Caffeine Decaffeinated tea and coffee Carbonated drinks Artificial sweeteners Corn syrup Foods that are high in spice, sugar or acid, especially citrus fruits Heart and blood pressure medications, sedatives, and muscle relaxants Large doses of vitamins B or C Urinary incontinence also may be caused by an easily treatable medical condition, such as: Urinary tract infection. Infections can irritate your bladder, causing you to have strong urges to urinate, and sometimes incontinence. Other signs and symptoms of urinary tract infection include a burning sensation when you urinate and foul-smelling urine. Constipation. The rectum is located near the bladder and shares many of the same nerves. Hard, compacted stool in your rectum causes these nerves to be overactive and increase urinary frequency. Persistent urinary incontinence Urinary incontinence can also be a persistent condition caused by underlying physical problems or changes, including: Pregnancy. Hormonal changes and the increased weight of the uterus can lead to stress incontinence. Childbirth. Vaginal delivery can weaken muscles needed for bladder control and also damage bladder nerves and supportive tissue, leading to a dropped (prolapsed) pelvic floor. With prolapse, the bladder, uterus, rectum or small intestine can get pushed down from the usual position and protrude into the vagina. Such protrusions can be associated with incontinence. Changes with age. Aging of the bladder muscle can decrease the bladder's capacity to store urine. Menopause. After menopause women produce less estrogen, a hormone that helps keep the lining of the bladder and urethra healthy. Deterioration of these tissues can aggravate incontinence. Hysterectomy. In women, the bladder and uterus are supported by many of the same muscles and ligaments. Any surgery that involves a woman's reproductive system, including removal of the uterus, may damage the supporting pelvic floor muscles, which can lead to incontinence. Enlarged prostate. Especially in older men, incontinence often stems from enlargement of the prostate gland, a condition known as benign prostatic hyperplasia. Prostate cancer. In men, stress incontinence or urge incontinence can be associated with untreated prostate cancer. But more often, incontinence is a side effect of treatments for prostate cancer. Obstruction. A tumor anywhere along your urinary tract can block the normal flow of urine, leading to overflow incontinence. Urinary stones — hard, stone-like masses that form in the bladder — sometimes cause urine leakage. Neurological disorders. Multiple sclerosis, Parkinson's disease, stroke, a brain tumor or a spinal injury can interfere with nerve signals involved in bladder control, causing urinary incontinence.

This is a video of a Gender Reassignment Surgery, watch as surgeons change a male to a female its an extremely interesting procedure
Any independent vertical movement of the transducer or the patient will affect the hydrostatic column of this fluid-filled system and thus alter the pressure measurements. At some time before or after PAC insertion, the system must therefore be zeroed to ambient air pressure. The reference point for this is the midpoint of the left atrium (LA), estimated as the fourth intercostal space in the midaxillary line with the patient in the supine position. With the transducer at this height, the membrane is exposed to atmospheric pressure, and the monitor is then adjusted to zero. Calibration Once zeroed, the monitoring system must be calibrated for accuracy. Currently, most monitors perform an automated electronic calibration. Two methods are used to manually calibrate and check the system. If the catheter has not been inserted, the distal tip of the PAC is raised to a specified height above the LA. For example, raising the tip 20 cm above the LA should produce a reading of approximately 15 mm Hg if the system is working properly (1 mm Hg equals 1.36 cm H 2 O). Alternatively, pressure can be applied externally to the transducer and adjusted to a known level using a mercury or aneroid manometer. The monitor then is adjusted to read this pressure, and the system is calibrated. Dynamic tuning Central pressures are dynamic waveforms (ie, they vary from systole to diastole) and thus have a periodic frequency. To monitor these pressures accurately, the system requires an appropriate frequency response. A poorly responsive system produces inaccurate pressure readings, and differentiating waveforms (eg, PA from pulmonary capillary wedge pressure [PCWP]) can become difficult. When signal energy is lost, the pressure waveform is dampened. Common causes of this are air bubbles (which are compressible), long or compliant tubing, vessel wall impingement, intracatheter debris, transducer malfunction, and loose connections in the tubing. A qualitative test of the frequency response is performed by flicking the catheter and observing a brisk high-frequency response in the waveform. After insertion, the system can be checked by using the rapid flush test. When flushed, an appropriately responsive system shows an initial horizontal straight line with a high-pressure reading. Once the flushing is terminated, the pressure drops immediately, which is represented by a vertical line that plunges below the baseline. A brief and well-defined oscillation occurs, followed by return of the PA waveform. A dampened system will not overshoot or oscillate, and causes a delay in returning to the PA waveform.

Childbirth (also called labour, birth, partus or parturition) is the culmination of a human pregnancy or gestation period with the birth of one or more newborn infants from a woman's uterus. The process of normal human childbirth is categorized in three stages of labour: the shortening and dilation of the cervix, descent and birth of the infant, and birth of the placenta. In many cases, with increasing frequency, childbirth is achieved through caesarean section, the removal of the neonate through a surgical incision in the abdomen, rather than through vaginal birth. In the U.S. and Canada it represents nearly 1 in 3 (31.8%) and 1 in 4 (22.5%) of all childbirths, respectively.
This minimally invasive procedure connects electrodes to the brain and places a pacemaker-like device under the skin. When activated, electrical impulses minimize shaking due to "dyskinesia syndrome" in patients with Parkinson's disease. ~ Detroit Medical Center
