- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This is how Paraumbilical hernia looks like and how it is examined although it looks very simple but in exam it can be very difficult to perform all steps in small amount of time. This can be short case or even long of #cpsp #fcps #mbbs #medicalstudent #mbbsexams #plab2 #plab #plab1 and MS #genernalknowledge #surgery exams
#para-umbilical hernia
#umbilical hernia #paraumbilical #hernia repair#laparoscopic paraumbilical hernia repair. #umbilical defect, #vetral hernia surgery. #herniatreatment #herniatreatment #ventral hernia hernia,#laparoscopic ventral hernia repair,umbilicus,carl lowe jr,hernia repair,training,north carolina,hernia repair surgery,charlotte,operation,laparoscopic,bulge,surgery,surgeon,dr. lowe,ipom repair,live surgery,mesh,
#mesh #ipom repair

Big Butt Abscess Drainage

#ComprehensiveClinicalClass
History, Examination and Management of Hernia
Mentor: Dr. Nishanth, Consultant Surgeon, Bengaluru.
THE WHITE ARMY
To make studies more interesting and enjoyable, we are constantly trying to share most important tables, charts, diagrams, mnemonics, scoring systems, diagnostic criterias, motivating quotes and other useful study materials on
ANDROID APP - All in 1 Free Medical Education App for Medicos
https://play.google.com/store/....apps/details?id=com.
INSTAGRAM PAGE
@the_whitearmy
https://www.instagram.com/the_whitearmy/
TELEGRAM GROUP
PDFs, PPTs and other study materials stored for easy, convenient access and download.
https://t.me/whitearmyofmedicos
Anyone interested to present clinical cases, willing to join whatsapp discussion group, can send a mail to whitearmyofmedicos@gmail.com
#StudyManiaInSocialMedia
#HelpOthersToHelpOurselves
#StudyEnjoyingEnjoyStudying
DISCLAIMER
THE WHITE ARMY does not own or claim to own any of the media used in the following video/stream. The media belong to their respective owners who may have copyright over them.The media have been taken from various sources and are used for medical educational purposes only. The following video/stream may contain images that may not be suitable for all audiences, viewer discretion is advised.
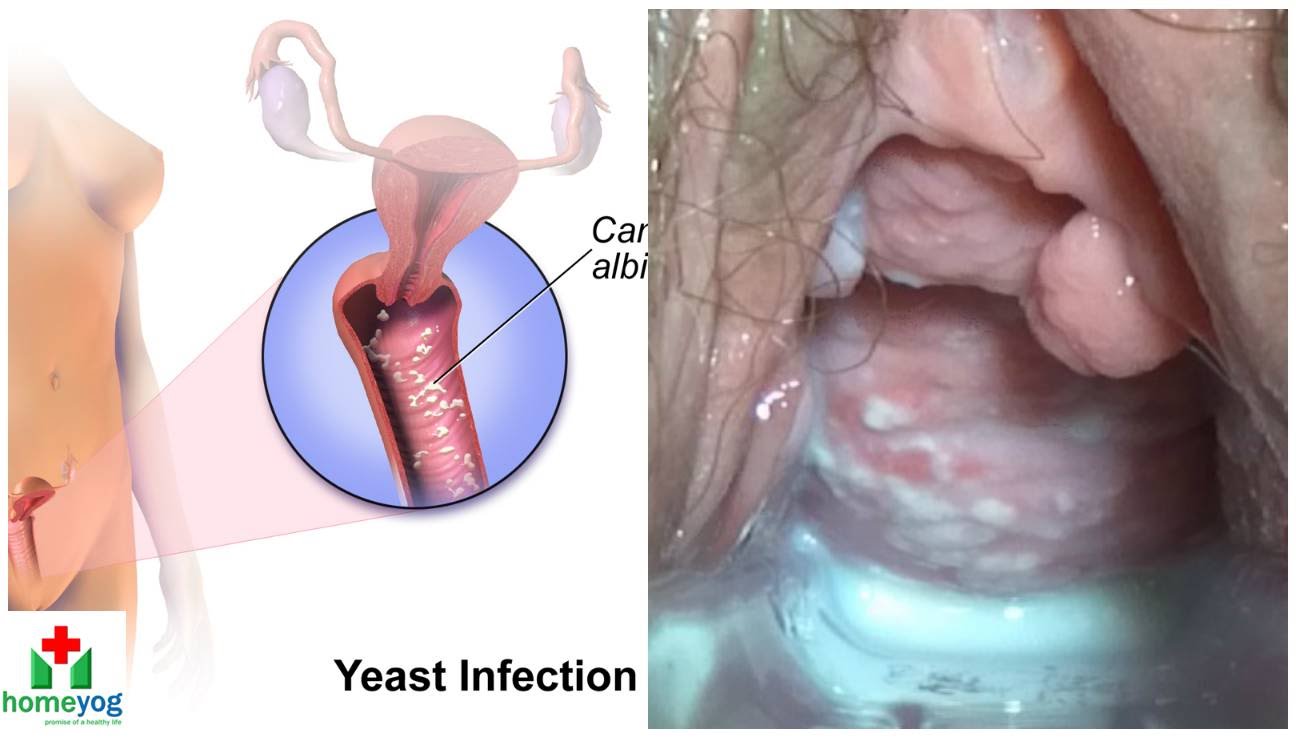
Watch that video to know the Female Genital Infections Causes and treatments.

A tummy tuck is a surgical process that removes excess fat and skin. Learn more about the procedure by watching this video!
Looking to book a consultation? Call Zuri Plastic Surgery now at 786-804-1603 or DM us today to schedule a complimentary consultation with Dr. Z.
Un tummy tuck es un procedimiento quirúrgico que elimina el exceso de grasa y piel. ¡Aprenda más sobre este procedimiento viendo este video!
¿Quiere agendar una consulta? Llame a Zuri Plastic Surgery ahora al 786-804-1603 o envíenos un DM hoy para programar una consulta gratuita con el Dr. Z.
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026

Patient Glenn Williams had a hernia measuring 20cm x 30cm. Consultant Graham Offer has performed ground breaking surgery to help Glenn.

Male and female Foley catheter insertion into bladder. Using mannequins.
The male orgasm is a common subject but usually misunderstood at the same time. Men are sometimes led to believe that ejaculating often is a bad thing, particularly if you masturbate. The truth is that ejaculation is important to every man due to a number of reasons. The main goal of this post is to shed some light on reasons why men need to ejaculate.

Majority of patients these days prefer PCNL ( Minimal Invasive Telescopic removal of kidney stones broken with lithoclast, removed through a button hole incision ). This patient with a big stone in the pelvis of the kidney wanted it open only so I did an open pyelolithotomy for this patient after a long time as I use to do it in routine in the past. Except for the long incision and scar as compared to PCNL the recovery time was the same and patient went home third day happily walking and eating.

► Get a free NCLEX NGN sample test today: http://lectur.io/nclexrnsampletestyt
► Create your free account today: http://lectur.io/nurseregisteryt
► If you’re an nursing educator or faculty member, visit: http://lectur.io/nursytb2u
In this video “How To Do An IM (Intramuscular) Injection” you will learn about:
►the steps in the administration of intramuscular medications
►the angle to position the syringe while administering an intramuscular injection
►the landmark to administer an intramuscular injection in the deltoid muscle
►5 tips for the safe administration of an intramuscular medication
►the steps of the Z-track method for intramuscular injections
►the role of aspirating blood during an intramuscular injection and evaluate whether this practice is currently in use
► This video is part of the Lecturio course “Fundamentals of Nursing: Clinical Skills”
► WATCH the complete course on http://lectur.io/njection
► THE PROF: Samantha Rhea MSN, RN has been a nurse since 2008 and a nursing faculty teacher since 2012. She has been recognized for clinical excellence as an interventional cardiology nurse and also led a Joint Commission Accredited Stroke Center. Ms. Rhea is an award-winning expert in clinical teaching and continues to maintain a current clinical practice and teaches at a University nursing program.
► LECTURIO is your smart tutor for nursing school: Learn the toughest NCLEX® topics with high-yield video lectures, integrated quiz questions, and more. Register now to study anytime and anywhere you want to: https://nursing.lecturio.com/#/
► CHECK OUT ALL NURSING COURSES:
Leadership Nursing: http://lectur.io/leadershipnursing
Dosage Calculation Nursing: http://lectur.io/dosagecalcnursing
Physiology Nursing: http://lectur.io/physiologynursing
Medical Surgical Nursing: http://lectur.io/medsurgnursing
Pharmacology Nursing: http://lectur.io/pharmacologynursing
NCLEX® Pharmacology Nursing: http://lectur.io/pharmnclexnursing
Pediatric Nursing: http://lectur.io/pediatricnursing
Study Skills Nursing: http://lectur.io/studyskillsnursing
Fundamentals of Nursing - Theory: http://lectur.io/fundamentalstheory
Fundamentals of Nursing - Clinical Skills: http://lectur.io/fundamentalsclinicalskills
Nursing Prerequisites: http://lectur.io/nursingprerequisites
Mental Health Nursing: http://lectur.io/mentalhealthnursing
Maternal-Newborn Nursing: http://lectur.io/maternalnewbornnursing
► INSTALL the free Lecturio app
iTunes Store: https://app.adjust.com/z21zrf
Play Store: https://app.adjust.com/b01fak
► SUBSCRIBE to our YouTube channel: http://lectur.io/subscribenursing
► WATCH MORE ON YOUTUBE: http://lectur.io/nursingplaylists
► LET’S CONNECT:
Facebook: www.facebook.com/lecturio.nursing
Instagram: www.instagram.com/lecturio_nursing
Join Discord Community: https://discord.gg/Ue95WDxCrp
TikTok: www.tiktok.com/@lecturio_nursing
LinkedIn: https://www.linkedin.com/company/lecturio-medical/
#nursingschool #nursingeducation #nursingclinicalskills #leadershipnursing #nclex #nursingfundamentals #nursingclinical #nursingskills
http://www.wss4m.com/vb

A hematoma is a collection of blood outside of a blood vessel. There are several types of hematomas and they are often described based on their location. Examples of hematomas include subdural, spinal, under the finger or toenail bed (subungual), ear, and liver (hepatic). Some causes of hematomas are as pelvic bone fractures, fingernail injuries (subungual), bumps, passing blood clots, blood clot in the leg (DVT), blood cancers, and excessive alcohol use. Symptoms of hematomas depend upon their location and whether adjacent structures are affected by the inflammation and swelling associated with the bleeding and may include

Ellis demonstrates how to perform a sterile wound dressing change. It would be appropriate to perform hand hygiene between glove changes.
Our Critical Nursing Skills video tutorial series is taught by Ellis Parker MSN, RN-BC, CNE, CHS and intended to help RN and PN nursing students study for your nursing school exams, including the ATI, HESI and NCLEX.
#NCLEX #ClinicalSkills #woundcare #HESI #Kaplan #ATI #NursingSchool #NursingStudent #Nurse #RN #PN #Education #LVN #LPN #nurseeducator
00:00 What to expect
00:51 Prepping for wound dressing change
1:15 Removing the old wound dressing
1:40 Assessing a wound
2:05 Setting up sterile field
2:49 Sterile gloving
4:02 Preparing equipment for wound dressing change
5:09 Cleaning a wound
6:13 Drying a wound
6:28 Packing a wound
7:19 Covering a wound
7:47 Labeling a wound dressing
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.

Delivery of the placenta
A video showing how to catheter the male urethra

Infected Tattoo Abscess

This is a diabetic foot ulcer. The patient reportedly went on vacation and noticed this ulcer upon their return. Debridement (removal of damaged tissue) to the level of healthy bleeding tissue is medically necessary as damaged tissue acts an impediment to wound healing. Due to their diabetic neuropathy, they did not feel any pain or indication that a wound was forming. This ulcer appeared to have penetrated to the level of subcutaneous tissue or even fascia, but turned out to be much deeper than that. These are serious wounds and are the beginnings of what lead to foot and leg amputations if they are not treated promptly by your healthcare provider, AKA Podiatrist.
Basic well-male examination of the genitals and digital rectal exam.

Wow! Ultrasound guided internal jugular vein cannulation (long axis approach)
