- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
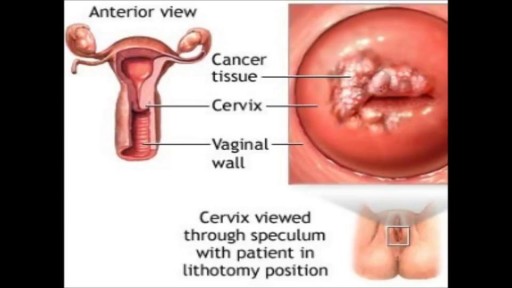
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Menorrhagia is the medical term for menstrual periods with abnormally heavy or prolonged bleeding. Although heavy menstrual bleeding is a common concern, most women don't experience blood loss severe enough to be defined as menorrhagia. With menorrhagia, you can't maintain your usual activities when you have your period because you have so much blood loss and cramping. If you dread your period because you have such heavy menstrual bleeding, talk with your doctor. There are many effective treatments for menorrhagia.
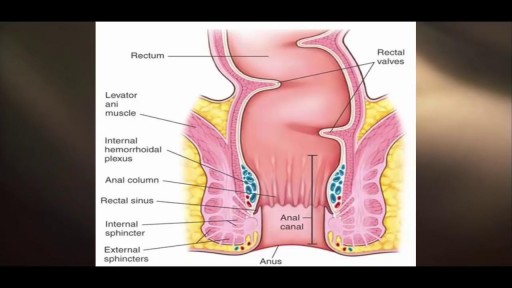
The only way to completely avoid anal sex risks is to abstain from anal sex. If you engage in anal sex, it is always important to use a condom to protect against the spread of infections and diseases.

Septic arthritis is also known as infectious arthritis, and is usually caused by bacteria, or fungus. The condition is an inflammation of a joint that's caused by infection. Typically, septic arthritis affects one large joint in the body, such as the knee or hip. Less frequently, septic arthritis can affect multiple joints
Although individual surgeons and centers employ different methods to insert a left ventricular assist device (LVAD), the fundamental concepts remain true for all. That is, most devices use the apex of the left ventricle (LV) as the inflow site to the pump, which subsequently gives off an outflow graft to the aorta, thus bypassing the ailing LV. Currently available devices do not differ significantly with regard to general implantation technique. The sequence of implantation can vary also from patient to patient, depending on the particular situation. In some cases, concomitant procedures may be performed in conjunction with LVAD implantation without adversely affecting outcome.
Caesarean section is the most common way to deliver a breech baby in the USA, Australia, and Great Britain. Like any major surgery, it involves risks. Maternal mortality is increased by a Caesarean section, but still remains a rare complication in the First World. Third World statistics are dramatically different, and mortality is increased significantly. There is remote risk of injury to the mother’s internal organs, injury to the baby, and severe hemorrhage requiring hysterectomy with resultant infertility. More commonly seen are problems with noncatastrophic bleeding, postoperative infection and wound healing problems. It should be added that the increase in maternal mortality rates could be slightly skewed due to the fact that Caesarean sections are often used during high-risk pregnancies and/or when mortality is already a strong possibility.
One large study has confirmed that elective cesarean section has lower risk to the fetus and a slightly increased risk to the mother, than planned vaginal delivery of the breech however elements of the methodology used have undergone some criticism.
The same birth injuries that can occur in vaginal breech birth may rarely occur in Caesarean breech delivery. A Caesarean breech delivery is still a breech delivery. However the soft tissues of the uterus and abdominal wall are more forgiving of breech delivery than the hard bony ring of the pelvis. If a Caesarean is scheduled in advance (rather than waiting for the onset of labor) there is a risk of accidentally delivering the baby too early, so that the baby might have complications of prematurity. The mother’s subsequent pregnancies will be riskier than they would be after a vaginal birth (uterine rupture). The presence of a uterine scar will be a risk factor for any subsequent pregnancies.

Each month inside your ovaries, a group of eggs starts to grow in small, fluid-filled sacs called follicles. Eventually, one of the eggs erupts from the follicle (ovulation). It usually happens about 2 weeks before your next period. Hormones Rise After the egg leaves the follicle, the follicle develops into something called the corpus luteum. The corpus luteum releases a hormone that helps thicken the lining of your uterus, getting it ready for the egg. The Egg Travels to the Fallopian Tube After the egg is released, it moves into the Fallopian tube. It stays there for about 24 hours, waiting for a single sperm to fertilize it. All this happens, on average, about 2 weeks after your last period.

Choking occurs when a foreign object becomes lodged in the throat or windpipe, blocking the flow of air. In adults, a piece of food often is the culprit. Young children often swallow small objects. Because choking cuts off oxygen to the brain, administer first aid as quickly as possible. The universal sign for choking is hands clutched to the throat. If the person doesn't give the signal, look for these indications: Inability to talk Difficulty breathing or noisy breathing Inability to cough forcefully Skin, lips and nails turning blue or dusky Loss of consciousness

Hematoma Removal! Surgery, Blood, Popping
The epididymis is a long coiled tube that lies above and behind each testicle. The epididymis collects and transports sperm from the testis to the vas deferens (tubes that transport sperm to the urethra). An epididymal cyst is a cyst-like mass in the epididymis that contains clear fluid. Typically, epididymal cysts and spermatoceles do not cause symptoms. When discovered, the epididymal cyst is usually about the size of a pea and feels separate from the top of the testis. Spermatoceles typically arise from the head of the epididymis, and are felt on the top portion of the testicle. Epididymal cysts and spermatoceles are often incidental findings on testicular self-examination or routine physical examination. It is important that any mass noted in the scrotum be examined by a urologist in order to obtain an accurate diagnosis, especially a mass on the testicle itself. Our team in the Division of Urology will typically be able to confirm the diagnosis on physical exam. However, a scrotal ultrasound may also be used in order to rule out other conditions.

Histology of Small Intestine Jejunum

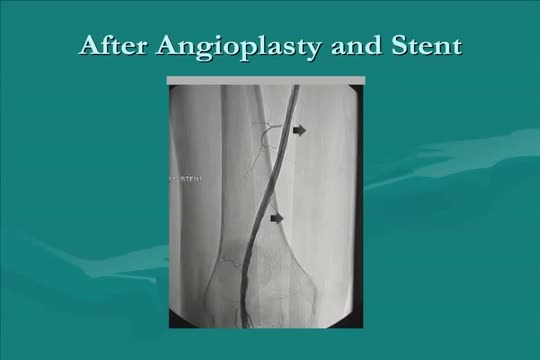
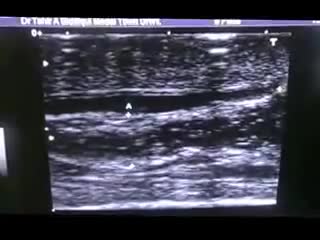
Roman Nowygrod, MD, a surgeon at NewYork-Presbyterian/Columbia University Medical Center, explains the different surgical approaches to treat Peripheral Arterial Disease (PAD).

Most people develop several moles (nevi) throughout adulthood. Moles can be found anywhere on the body, usually in sun-exposed areas, and are usually brown, smooth, and slightly raised. In most cases, a nevus is benign and doesn't require treatment. Rarely, they turn into melanoma or other skin cancers. A nevus that changes shape, grows bigger, or darkens should be evaluated for removal.

External cephalic version is a process by which a breech baby can sometimes be turned from buttocks or foot first to head first. External cephalic version (ECV) is a manual procedure that is advocated by national guidelines for breech presentation singleton pregnancy, in order to enable vaginal delivery.
Erectile dysfunction (ED) is the inability to get or keep an erection firm enough for sexual function. It’s a common sexual problem, affecting as many as 30 million men in the United States. Most cases of ED have a physical cause, such as heart disease, diabetes, and obesity. Lifestyle choices like smoking and drinking excessive amounts of alcohol can also lead to ED. But for some men, psychological issues are the root of the problem.

This 35 years old man lost his right wrist in metal lathe cut machine. the video is taken about 2 years after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic

Urinary tract infections (UTIs) are infections of the urethra, bladder, ureters, or the kidneys, which comprise the urinary tract. E. coli bacteria cause the majority of UTIs, but many other bacteria, fungi, and parasites may also cause UTIs. Females have a higher risk for UTIs than most males, probably because of their anatomy; other risk factors for UTIs include any condition that may impede urine flow (e.g., enlarged prostate, kidney stones, congenital urinary tract abnormalities, and inflammation). Patients with catheters or those who undergo urinary surgery and men with enlarged prostates are at higher risk for UTIs.
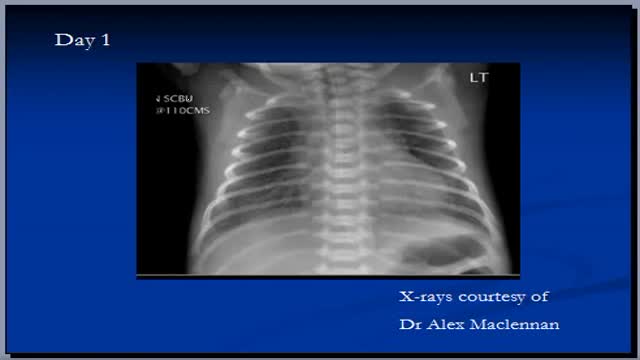
The video will describe RDS in premature babies. Please see website for disclaimer

All Solution of Male Disorder Male Infertility Diagnostic and Treatment Re-Slim Care Latest Technology in Pakistan Dr. Aslam Naveed is a well known sexologist in Pakistan. He has treated more than 1 Lac patients since last 30 years of clinical Practice in sexology, he knows how to help the people facing sexual disorders. Contact: 02134965050, 03432821919, 0345-8314663 http://www.sexologistpakistan.com/ https://www.facebook.com/menssexcareclinic/ https://www.youtube.com/channel/UCagSSgdEgQJWl_xfFM12BwA https://twitter.com/bettersexcare https://www.instagram.com/dr.aslamnaveed/ ADDRESS: Men’s Care Modern Hospital, Opposite, Safari Park, University Road, Karachi, Pakistan.
