- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Ptosis is when the upper eyelid droops over the eye. The eyelid may droop just a little, or so much that it covers the pupil (the black dot at the center of your eye that lets light in). Ptosis can limit or even completely block normal vision. Children and adults can have ptosis. Fortunately, this condition can be treated to improve vision as well as appearance.

#GIT#Abdominalexamination#AETCM

Pediatric Urine Samples Collection

Knee reflex video from the USMLE collection

.

Watch that video of The Biggest Ingrown Hair Removed

Patients are generally placed in a supine position with the head in an extended position. As noted above, Gardner-Wells tongs can be used for additional cervical traction. The hands can also be tied downward to increase the operative exposure. Once the surgical site is properly prepared with cleansing material, the appropriate surgical level is identified with intraoperative radiographs. A scalpel is used to make a linear longitudinal incision just medial to the body of the sternocleidomastoid muscle. The incision is made long enough to include at least 2 vertebral levels if a 1-level discectomy is being performed. Alternatively, transverse skin incisions over the targeted vertebral level can also be performed. The platysmal muscle is identified and incised. The platysmal incision can be extended if a multilevel decompression is the surgical aim. Extensive subplatysmal dissection is performed to reduce retraction injury.
Egg Freezing Oocyte Cryopreservation


This covers some of the benefits, side effects and potential complications of LASIK Eye Surgery! Learn about the pros and cons of laser eye surgery and some pro tools to help you along the way.
📒 Show Notes and Resources 📒
LASIK Affordability Calculator
http://www.refractivealliance.....com/lasik-affordabil
Patient Guide to Refractive Surgery
https://www.aao.org/Assets/e89....0eb55-9bfa-465a-8422
Some Reference Articles for you folks who like to read
https://www.healio.com/ophthal....mology/journals/jrs/
Dry Eye Playlist
https://www.youtube.com/playli....st?list=PLzi60fSuOmP
---------My Cameras and Video Gear -------
https://kit.co/DoctorEyeHealth
DISCLAIMER: Some of the links in this description are "affiliate links", a link with a special tracking code. This means if you click on an affiliate link and purchase the item, I may receive an affiliate commission. Regardless, I only recommend products or services I believe will add value to viewers.
======================================================
Let’s Connect! Dr. Allen on Social Media:
https://instagram.com/doctoreyehealth
https://www.facebook.com/doctoreyehealth
https://twitter.com/doctoreyehealth
For Collaborations please email me: DoctorEyehealth@gmail.com
MEDICAL ADVICE DISCLAIMER: All content in this video and description including: information, opinions, content, references and links is for informational purposes only. The Author does not provide any medical advice on the Site. Accessing, viewing, reading or otherwise using this content does NOT create a physician-patient relationship between you and it’s author. Providing personal or medical information to the Principal author does not create a physician-patient relationship between you and the Principal author or authors. Nothing contained in this video or it’s description is intended to establish a physician-patient relationship, to replace the services of a trained physician or health care professional, or otherwise to be a substitute for professional medical advice, diagnosis, or treatment. You should consult a licensed physician or appropriately-credentialed health care worker in your community in all matters relating to your health.
About:
In this video you will find a laser eye surgery review. We cover the laser eye surgery procedure and how lasik eye surgery works. A large emphasis is on the benefits of laser eye surgery as well as potential side effects and complications. We even touch on the topic of lasik eye surgery gone wrong.
#lasikeyesurgery #lasiksurgery #lasik

Pregnancy Stretch Marks Removal Treatment

Watch that video of a Man With Pipe Penetrated His Head Inside Emergency Room

Could this be a viable alternative to open heart surgery?

It sounds like you're questioning whether or not your water may have broken, and this can actually be a hard thing for a lot of women to tell. Usually if your water breaks, it's just a trickle of fluid, and you're afraid to admit it to anyone because you think you peed your pants. And it is normal to pee your pants when you're pregnant because the bladder is right below the uterus, and if the baby moves just right, it might kick out a little bit of urine. So if you feel a trickle or a little tiny gush of fluid, what you want to do is put a pad or a pantie-liner on after going to the bathroom and emptying your bladder, and wait an hour and see if fluid continues to come out. And if it does, then you're not having bladder leakage issues - your water is probably broken.

Mesenteric Vessel Ligation

A local doctor says that the new pap smear guidelines makes sense for many women
Amazing animation: General Dentistry in 3D
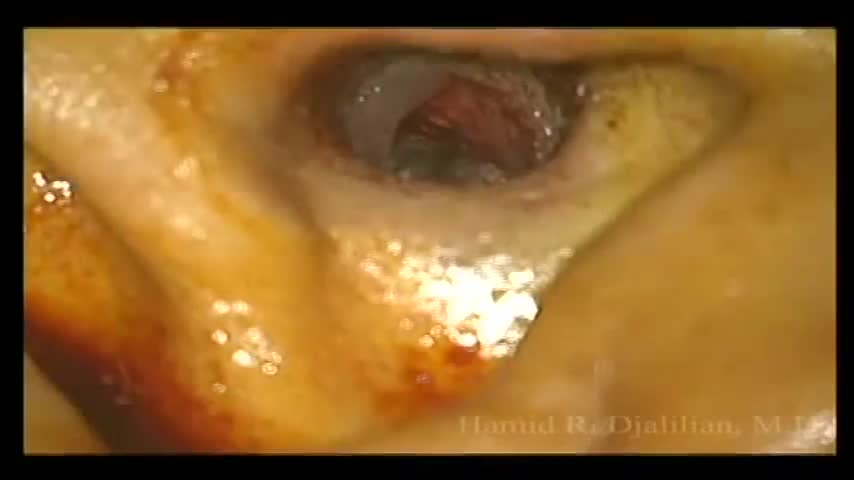
This is a surgery showing the removal of a large exostosis. Exostoses are bony growths in the ear canal from chronic exposure to cold water/air, most commonly from surfing. This patient had growths in both ears, which were completely obstructing the ear canals. This patient had a single exostosis that was blocking this side (the right side).

Choking occurs when a foreign object becomes lodged in the throat or windpipe, blocking the flow of air. In adults, a piece of food often is the culprit. Young children often swallow small objects. Because choking cuts off oxygen to the brain, administer first aid as quickly as possible. The universal sign for choking is hands clutched to the throat. If the person doesn't give the signal, look for these indications: Inability to talk Difficulty breathing or noisy breathing Inability to cough forcefully Skin, lips and nails turning blue or dusky Loss of consciousness

Dental Abscess Drainage and Extraction
