- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Indwelling urinary catheters are commonly used in hospitals and can lead to preventable catheter-associated UTI. How can rates of catheter-associated UTI be reduced in hospitals? New research findings are summarized in a new NEJM Quick Take. Learn more at http://nej.md/1WoeHdF SHOW MORE
Hip Resurfacing Surgery Videos Welcome to the website of the Asian Regional Center for Hip Resurfacing (ARCH) is a specialized surgical center in Apollo Speciality Hospital Chennai. More than 1350 Hip Resurfacing Surgeries have been performed so far. Asian Regional Center for Hip Resurfacing is the first specialized resurfacing center in Asia. Patients with arthritis and hip pain travel from all over the world travel to ARCH for hip surgery. Hip Resurfacing Surgery has revolutionized hip arthroplasty especially for younger and active patients. Unlike conventional Total Hip Replacement (THR) the hip resurfacing conserves the bone in the hip which would be crucial in younger patients. No restrictions are imposed on the resurfaced hip and the patient can participate in any professional or recreational activity after the surgery.

This surgery is usually done while you are under general anesthesia. That means you will be asleep and pain-free. Healthy skin is taken from a place on your body called the donor site. Most people who are having a skin graft have a split-thickness skin graft. This takes the two top layers of skin from the donor site (the epidermis) and the layer under the epidermis (the dermis). The donor site can be any area of the body. Most times, it is an area that is hidden by clothes, such as the buttock or inner thigh. The graft is carefully spread on the bare area where it is being transplanted. It is held in place either by gentle pressure from a well-padded dressing that covers it, or by staples or a few small stitches. The donor-site area is covered with a sterile dressing for 3 to 5 days. People with deeper tissue loss may need a full-thickness skin graft. This requires an entire thickness of skin from the donor site, not just the top two layers. A full-thickness skin graft is a more complicated procedure. Common donor sites for full-thickness skin grafts include the chest wall, back, or abdominal wall.
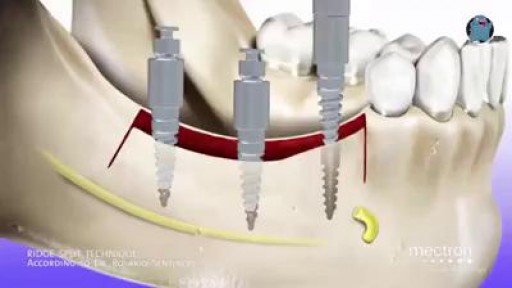
Ridge splitting with bone expansion is a technique of manipulation of bone to form receptor site for implant without removing any bone from the implant site.
Papillary fibroelastoma is the third most common primary tumor of the heart and is most likely to involve the cardiac valves. Like myxomas, they arise from the endocardium in most patients and since these tumors are often incidental findings at echocardiography or autopsy, the true incidence is difficult to estimate. Most patients are older than 60 years, which also contrasts with myxomas. Papillary fibroelastomas can embolize, leading to severe neurological complications and therefore, surgical removal is advised, although there is controversy regarding small incidental lesions and the need for surgery.


Watch that Hemorrhoids Repairing Medical Video

Otto Placik MD. a board certified Chicago Illinois based plastic surgeon presents instructional video on post genital surgery (labia minora reduction aka labiaplasty or labioplasty or clitoral hood reduction) massage exercises for treatment of labum minora psot surgical fibrosis or hypersensitivity. Photos pictures and video of anatomic models are reviewed . Great for patients thinking about or planning labiaplasty or vaginal cosmetic surgery

35 year old women with breathing difficulties for 6 months and feels like fluid is leaking down her front and back. Pain in thorax, lower back and pelvic. Weight loss. Was exposed to mold for a 2 years. Has a dog witch has persistent worm infection. Also been traveling out of the country.
Methotrexate works by reducing the function of the cells that are causing inflammation in the joint tissues. "Its use can reduce inflammation and therefore should help relieve pain and protect from joint damage," notes Sean A. Whelton, MD, a rheumatologist and associate professor of medicine at MedStar Georgetown University Hospital in Washington, D.C. Less inflammation in the joints should mean less joint pain and less joint swelling. You should also feel less fatigue and less morning stiffness.
مرکز ایمپلنت و زیبایی دندان شیراز دکتر محمد امین دین پرور

Trying to survive medical school funny video
Prostate Health and Cancer Seminar features nationally renowned physicians and scientists presenting the most current study and practices for the diagnosis and treatment of prostate cancer. This day-long program offers in-depth exploration of prostate issues that range from monitoring PSA counts to cutting-edge research to current treatment trends.
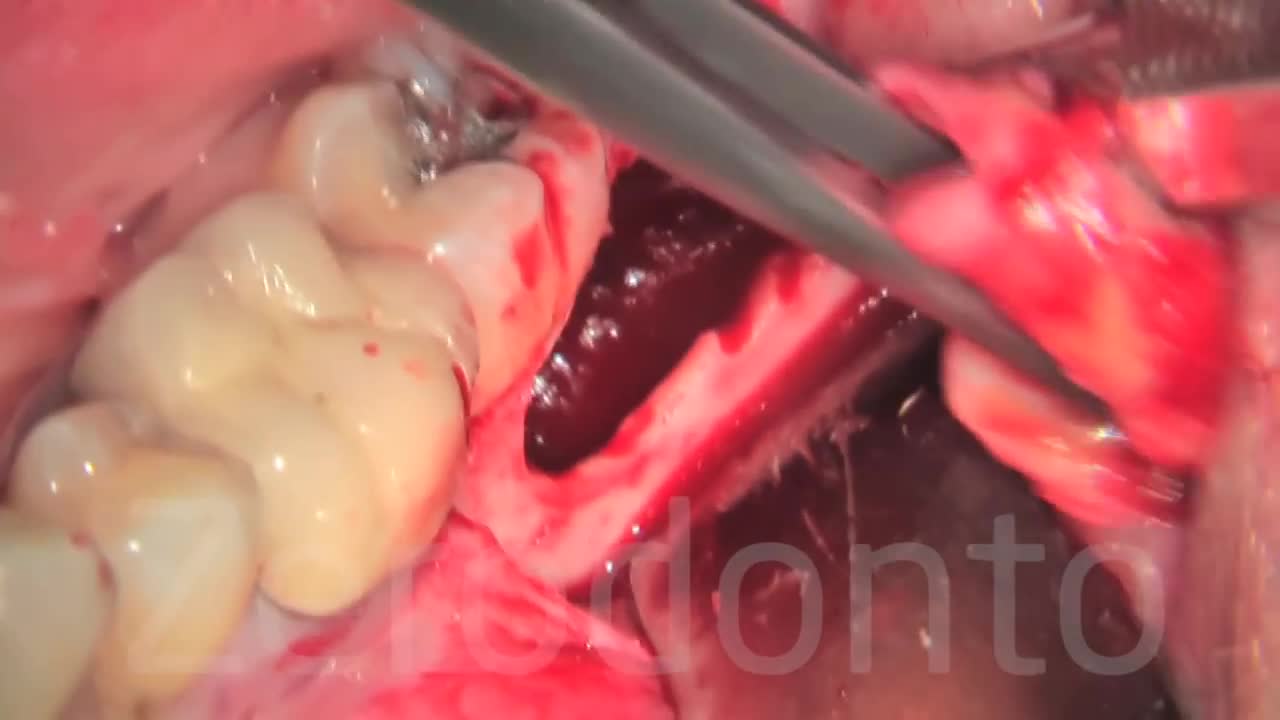
This pressure can also cause problems with crowding of the other teeth or require orthodontic treatment to straighten other teeth. Cysts. The wisdom tooth develops in a sac within the jawbone. The sac can fill with fluid, forming a cyst that can damage the jawbone, teeth and nerves.

Traumatic penile injury can be due to multiple factors. Penile fracture, penile amputation, penetrating penile injuries, and penile soft tissue injuries are considered urologic emergencies and typically require surgical intervention. The goals of treatment for penile trauma are universal: preservation of penile length, erectile function, and maintenance of the ability to void while standing. Traumatic injury to the penis may concomitantly involve the urethra.[1, 2] Urethral injury and repair is beyond the scope of this article but details can be found in Urethral Trauma. Penile fracture Penile fracture is the traumatic rupture of the corpus cavernosum. Traumatic rupture of the penis is relatively uncommon and is considered a urologic emergency.[3] Sudden blunt trauma or abrupt lateral bending of the penis in an erect state can break the markedly thinned and stiff tunica albuginea, resulting in a fractured penis. One or both corpora may be involved, and concomitant injury to the penile urethra may occur. Urethral trauma is more common when both corpora cavernosa are injured.[4] Penile rupture can usually be diagnosed based solely on history and physical examination findings; however, in equivocal cases, diagnostic cavernosography or MRI should be performed. Concomitant urethral injury must be considered; therefore, preoperative retrograde urethrographic studies should generally be performed. See the images below.
Genital warts are growths on the skin of the genital area and around the anus. They are caused by certain types of the human papilloma virus (HPV). There are more than 100 types of HPV. Some types of HPV produce warts on different parts of the body, like plantar warts on the feet and common hand warts. There is no specific treatment for HPV, but there are treatments for health problems caused by HPV. Genital warts can be treated by your healthcare provider, or with prescription medication. HPV-related cancers are more treatable when diagnosed and treated promptly. For more information, visit www.cancer.org.
Integrative Physical Examination Lecture
