- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
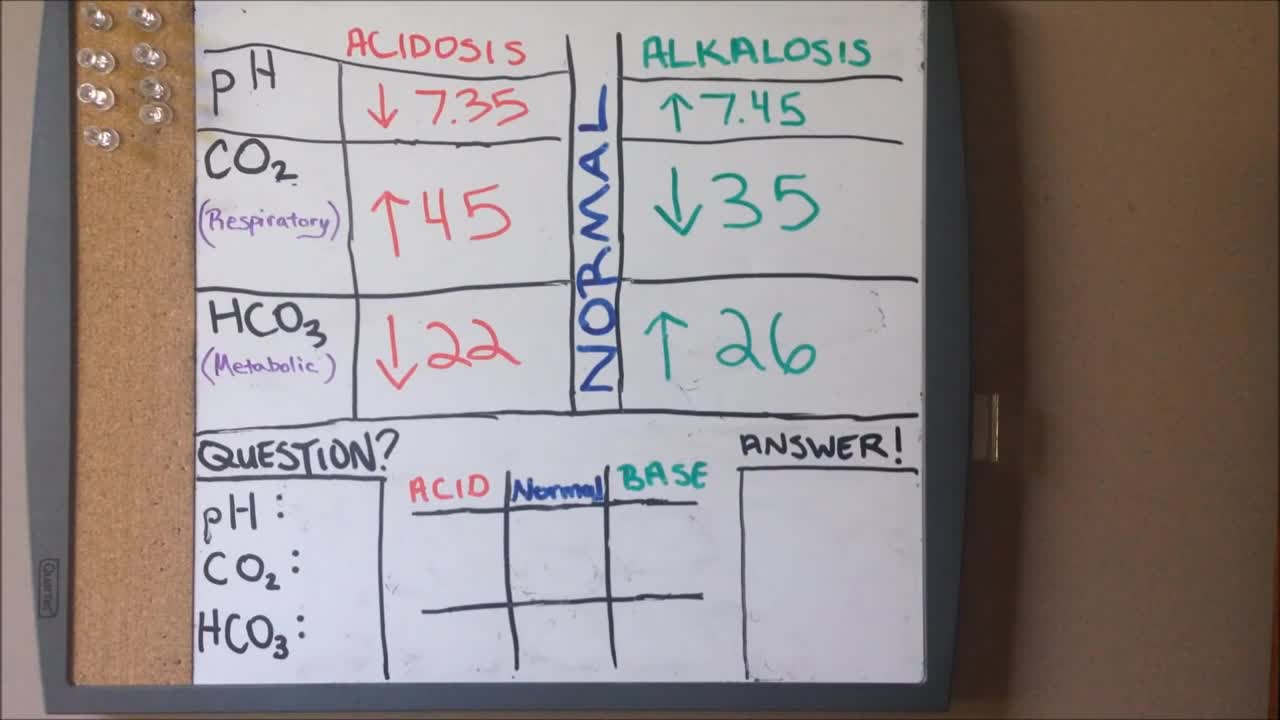
ABGs Made Easy | Arterial Blood Gas | Acid Base Balance: Everything You Need To Know!

The obstetric examination is distinct from other examinations in that you, the clinician, are trying to assess the health of two individuals – the mother and the fetus – simultaneously. From the initial history, you should be able to judge the health of the pregnancy, any risk factors that need to be addressed, and any concerns from the parents. The history is an opportunity for you to find out how much the parents know about pregnancy, labour and delivery and if they have any preferences to which these events are carried out. A carefully taken history will also direct your attention to specific signs during the examination. As such, it is important that you develop a concise and systematic method of taking the history and carrying out the examination so that you do not miss any important information. This article focuses primarily on the examination. Pregnancy is a sensitive issue, especially for the primigravida’s. Therefore, extra care is needed when you approach a pregnant woman. Always obtain expressed informed consent before examining her and have a chaperone accompany you throughout the examination. A walk-through of what you will be doing is a good way of reassuring the patient and allows the examination to go on smoothly. It is also important to let your patient know that if the examination is too painful, she can stop at any time she wants. Finally, before you begin, you should always wash your hands, especially at an OSCE station.
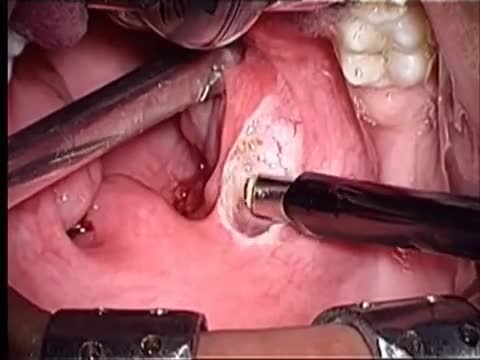
Tonsillectomy using coblation technique by wand Evac 70
Egg Freezing Oocyte Cryopreservation
Transvenous cardiac pacing, also called endocardial pacing, is a potentially life saving intervention used primarily to correct profound bradycardia. It can be used to treat symptomatic bradycardias that do not respond to transcutaneous pacing or to drug therapy.

Bone Movement During Childbirth and Delivery 3D

management of the second stage of labour

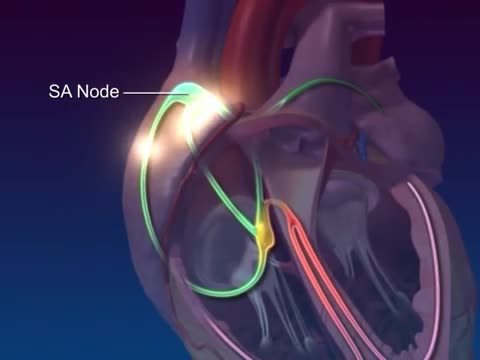
The cardiac conduction system is a group of specialized cardiac muscle cells in the walls of the heart that send signals to the heart muscle causing it to contract. The main components of the cardiac conduction system are the SA node, AV node, bundle of His, bundle branches, and Purkinje fibers.

Nasal polyps are linked to allergic rhinitis, asthma, aspirin allergy, sinus infections, acute and chronic infections, something stuck in the nose, and cystic fibrosis. But many times the cause is unknown. Sometimes, people get them before they develop asthma or sinusitis
What is a brain aneurysm? A brain (cerebral) aneurysm is a bulging, weak area in the wall of an artery that supplies blood to the brain. In most cases, a brain aneurysm causes no symptoms and goes unnoticed. In rare cases, the brain aneurysm ruptures, releasing blood into the skull and causing a stroke. When a brain aneurysm ruptures, the result is called a subarachnoid hemorrhage. Depending on the severity of the hemorrhage, brain damage or death may result.

The gastric balloon procedure (endoscopic intragastric balloon) leaves an inflated silicon balloon in the stomach for 6 months, making less room for food. As a result, patients: Feel full sooner while eating and therefore eat less. Lose about 30% of their excess weight in 6 months.

stage of pregnancy 2016

This video may contain images of a medical doctor providing emergency care for a patient.

Most times, a pulmonary embolism is caused by blood clots that travel from the legs or, rarely, other parts of the body (deep vein thrombosis, or DVT). Symptoms include shortness of breath, chest pain, and cough. Prompt treatment to break up the clot greatly reduces the risk of death. This can be done with blood thinners and drugs or procedures. Compression stockings and physical activity can help prevent clots from forming in the first place.
An excerpt from the award-winning documentary “Exposure: Environmental Links to Breast Cancer” about the effects of radiation. Featuring Olivia Newton-John, Dr. Rosalie Bertell and Dr. Susan Love.

Watch that Mid Palm Amputated Hand Reattachment Medical Surgery

Tough to beat! Head #InsideTheOR with S. Christopher Malaisrie, MD, and witness open heart surgery by one of the best cardiology and heart surgery programs in the nation as ranked by US News and World Report.

LASIK eye surgery is commonly performed laser refractive surgery to correct vision problems. This 3d animation shows how laser-assisted in situ keratomileusis (lasik) can be an alternative to glasses or contact lenses.
It’s one of many vision correction surgeries that work by reshaping your cornea, the clear front part of your eye, so that light focuses on the retina in the back of your eye.
In eyes with normal vision, the cornea bends (refracts) light precisely onto the retina at the back of the eye. But with nearsightedness (myopia), farsightedness (hyperopia) or astigmatism, the light is bent incorrectly, resulting in blurred vision.
During LASIK surgery, a special type of cutting laser is used to precisely change the shape of the dome-shaped clear tissue at the front of your eyes (cornea) to improve vision.
Glasses or contact lenses can correct vision, but reshaping the cornea itself also will provide the necessary refraction.
For more information about medical animation, please visit https://www.amerra.com
Watch more medical animations:
Craniectomy brain surgery - 3D animation: https://youtu.be/1RkseDeYS9g
Accessing an implantable port training - 3D animation: https://youtu.be/xSTpxjyv4O4
Open Suctioning with a Tracheostomy Tube - 3D animation: https://youtu.be/wamB7jpWCiQ
Ventriculostomy Brain Surgery - 3d animation: https://youtu.be/pUy0YDzVNzs
Suctioning the endotracheal tube - medical animation: https://youtu.be/pN6-EYoeh3g
Functional endoscopic sinus surgery (FESS) - 3D animation: https://youtu.be/qKTRyowwaLA
How to insert a nasogastric tube for NG intubation - 3d animation: https://youtu.be/Abf3Gd6AaZQ
Oral airway insertion - oropharyngeal airway technique - 3D animation: https://youtu.be/caxUdNwjt34
Nasotracheal suctioning (NTS) - 3D animation: https://youtu.be/979jWMsF62c
Learn about hemorrhoids with #3d #animation: https://youtu.be/R6NqlMpsiiY
CPR cardiopulmonary resuscitation - 3D animation: https://youtu.be/G87knTZnhks
What are warts (HPV)? - 3D animation: https://youtu.be/guJ1J7rRs1w
How Macular Degeneration Affects Your Vision - 3D animation: https://youtu.be/ozZQIZ_52YY
NeoGraft hair transplant procedure – animation: https://youtu.be/C-eTdH2UPXI

Dental implant surgery
