- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Intra-abdominal abscess continues to be an important and serious problem in surgical practice. Appropriate treatment is often delayed because of the obscure nature of many conditions resulting in abscess formation, which can make diagnosis and localization difficult. Associated pathophysiologic effects may become life threatening or lead to extended periods of morbidity with prolonged hospitalization. Delayed diagnosis and treatment can also lead to increased mortality; therefore, the economic impact of delaying treatment is significant.

Squats are one of the essential exercises to do during pregnancy there are so many benefits from doing this functional type of exercise. Strengthening your glute muscles, that's your butt, helps to decrease lower back and pelvic pain.
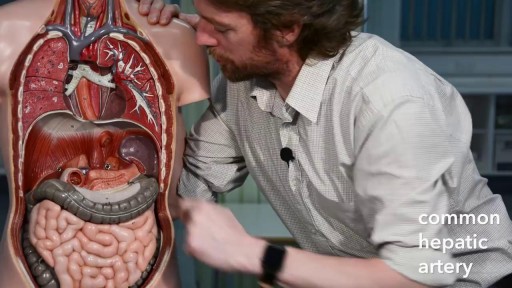
The primary functions of the liver are: Bile production and excretion. Excretion of bilirubin, cholesterol, hormones, and drugs. Metabolism of fats, proteins, and carbohydrates. Enzyme activation. Storage of glycogen, vitamins, and minerals. Synthesis of plasma proteins, such as albumin, and clotting factors.
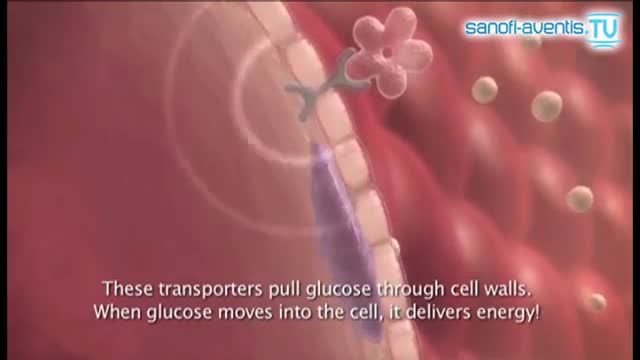
Insulin is a hormone made naturally in the pancreas that helps move sugar into the cells of your body. Your cells use the sugar as fuel to make energy. Without enough insulin, sugar stays in your bloodstream, raising your blood sugar. High blood sugar, or hyperglycemia, can lead to the signs and symptoms of diabetes:
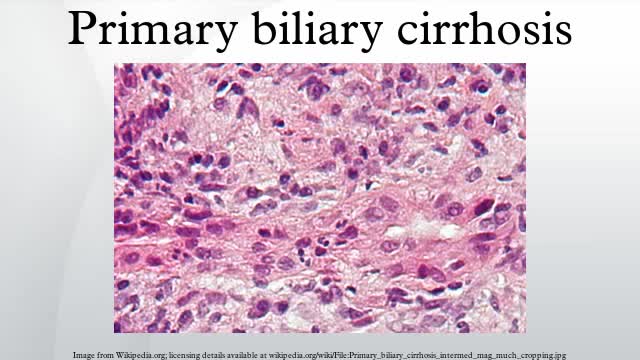
Primary biliary cirrhosis, sometimes called PBC, is a disease in which the bile ducts in your liver are slowly destroyed. Bile, a fluid produced in your liver, plays a role in digesting food and helps rid your body of worn-out red blood cells, cholesterol and toxins. When bile ducts are damaged, as in primary biliary cirrhosis, harmful substances can build up in your liver and sometimes lead to irreversible scarring of liver tissue (cirrhosis). Primary biliary cirrhosis is considered an autoimmune disease, in which the body turns against its own cells. Researchers think it is triggered by a combination of genetic and environmental factors. Primary biliary cirrhosis usually develops slowly and medication can slow its progression, especially if treatment begins early.

Juvenile polyposis syndrome (JPS) is a hereditary condition that is characterized by the presence of hamartomatous polyps in the digestive tract. Hamartomas are noncancerous (benign) masses of normal tissue that build up in the intestines or other places. These masses are called polyps if they develop inside a body structure, such as the intestines. The term “juvenile polyposis” refers to the type of polyp (juvenile polyp) that is found after examination of the polyp under a microscope, not the age at which people are diagnosed with JPS.

Orthopedic spine surgeons and vascular surgeons at UW Health in Madison, WI work together to perform minimally invasive anterior lumbar interbody fusion (Mini-ALIF). With this type of spinal fusion surgery, patients have smaller incisions, usually spend less time in the hospital and typically return to daily activities more quickly. Learn more https://www.uwhealth.org/ALIF
Barium Enema
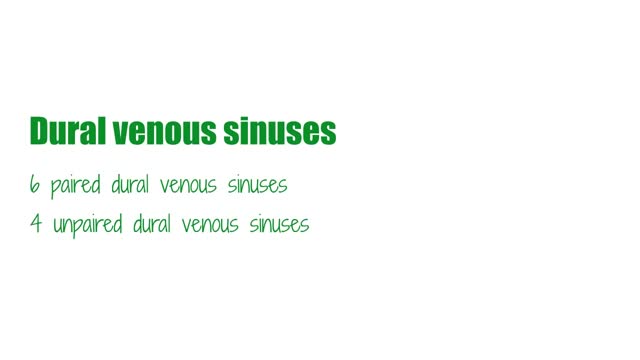
The superior sagittal sinus (also known as the superior longitudinal sinus), within the human head, is an unpaired area along the attached margin of falx cerebri. It allows blood to drain from the lateral aspects of anterior cerebral hemispheres to the confluence of sinuses.

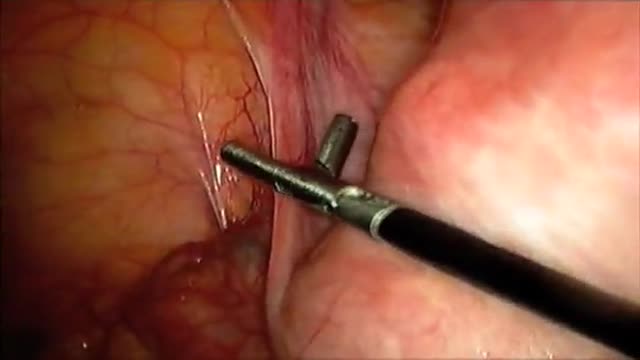
popliteal embolectomy; medial approach using a 4 f fogarty catheter

Vatche, Minassian, MD, MPH, Chief of Urogynecology, and Sarah Cohen, MD, MPH, Director of the Minimally Invasive Gynecologic Surgery Fellowship Program at Brigham and Women’s Hospital, perform a laparoscopic burch colposuspension, a procedure used to correct stress urinary incontinence.
Stress urinary incontinence is one of the most common types of incontinence and is characterized by urinary leakage during physical activities including coughing, sneezing, exercising, lifting, and laughing. As the condition progresses, it can become severe enough to happen with simple acts such as bending and walking. This condition is due to an anatomic weakness of the bladder neck which typically maintains the seal of urine during activity. Stress incontinence can result from a variety of conditions including vaginal childbirth, aging, menopause and obesity. As this is an anatomic condition, primary treatment may involve pelvic floor exercises and/or minimally invasive surgery.
Learn more about treatment for stress urinary incontinence:
Division of Urogynecology: http://www.brighamandwomens.or....g/Departments_and_Se
Division of Minimally Invasive Gynecologic Surgery: http://www.brighamandwomens.or....g/Departments_and_Se

Amazing Lung Inflation

腹腔镜联合胆囊+阑尾切除术——普外寰潮网,汕头市第二人民医院

How to push a baby out video how to prevent tearing during labor and delivery
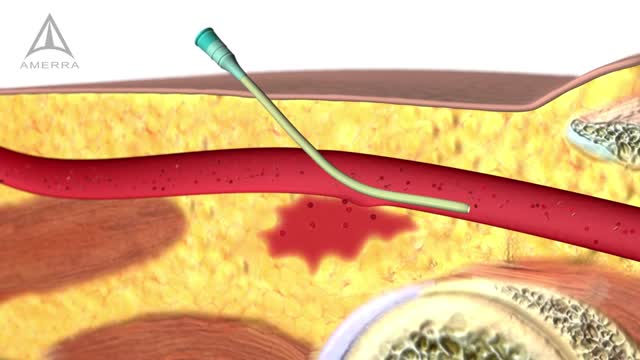
Internal Bleeding Detection
Testosterone treatment in adolescent boys with constitutional delay
Laparoscopic Supracervical Hysterectomy

Have you heard any medical lingo you've thought is strange? Funny healthcare speaker Dr. Brad Nieder discusses funny medical terminology he's learned in his medical career. He brings his medical comedy to a healthcare conference, describing how he didn't know what "stat" meant.
He goes on about how he thought up many funny terms he could say in return to the doctor who introduced him to the word. His healthcare comedy makes the crowd burst with laughter.
Dr. Brad knows how to adapt his hilarious real-life stories into customized presentations for any in-person or virtual event. Watch more of his videos as a medical comedian and all-around funny guy by browsing his videos.

USMLE Step 2 CS - Amenorrhea - This is just preview video. To get full access please visit our website : www.usmletutoring.com
