- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

EART (Health Education and Rescue Training) Wilderness First Aid is an intensive course that covers patient examination and evaluation, body systems and anatomy, wound care, splinting, environmental emergencies, and backcountry medicine. Hands-on simulations provide first-hand training in treating patients. This is an excellent course taught by experienced Wilderness First Responders and Emergency Medical Technicians and is highly recommended to all wilderness travelers. People who pass the courses will receive a Wilderness First Aid certification from the Emergency Care and Safety Institute (ECSI) which is good for 2 years. Participants who successfully pass CPR and HEART Wilderness First Aid will have met the First Aid requirements for OA Leader Training.


Gonorrhea is a sexually transmitted disease (STD). It’s caused by infection with the bacterium Neisseria gonorrhoeae. It tends to infect warm, moist areas of the body, including the: urethra (the tube that drains urine from the urinary bladder) eyes throat vagina anus female reproductive tract (the fallopian tubes, cervix, and uterus) Gonorrhea passes from person to person through unprotected oral, anal, or vaginal sex. People with numerous sexual partners or those who don’t use a condom are at greatest risk of infection. The best protections against infection are abstinence, monogamy (sex with only one partner), and proper condom usage. Behaviors that make a person more likely to engage in unprotected sex also increase the likelihood of infection. These behaviors include alcohol abuse and illegal drug abuse, particularly intravenous drug use.

the motor milestones expected in typically developing babies, from head control to walking and what pediatricians look for during a well-baby visit. She also explains the specific types of motor control a baby must master before the next milestone can be achieved

Robot Flies Like a Bird
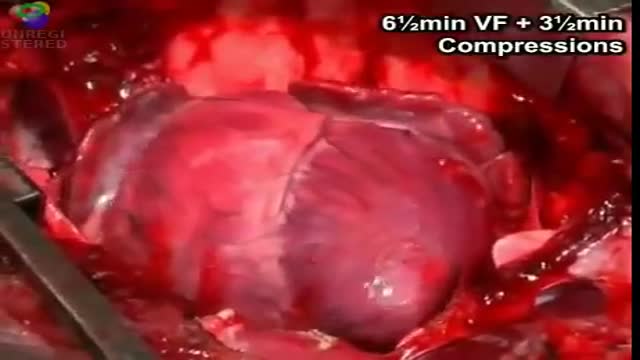
cardiac massage intermittent compression of the heart by pressure applied either over the sternum (closed cardiac massage) or directly to the heart through an opening in the chest wall (open cardiac massage). simple massage in the nursing interventions classification, a nursing intervention defined as stimulation of the skin and underlying tissues with varying degrees of hand pressure to decrease pain, produce relaxation, and/or improve circulation.

Watch that video of Closing Ejaculation Canal to Stop Sperm Surgery
Sickle cell anemia (sickle cell disease) is a disorder of the blood caused by an inherited abnormal hemoglobin (the oxygen-carrying protein within the red blood cells). The abnormal hemoglobin causes distorted (sickled) red blood cells.

Dialysis Fistula clip from full video on Dialysis Options
Overactive bladder syndrome is common. Symptoms include an urgent feeling to go to the toilet, going to the toilet frequently and sometimes leaking urine before you can get to the toilet (urge incontinence). Treatment with bladder training often cures the problem. Sometimes medication may be advised in addition to bladder training to relax the bladder.

How to Remove Blackhead from the Face
Cytomegalovirus (CMV) is a common virus that can infect almost anyone. Most people don't know they have CMV because it rarely causes symptoms. However, if you're pregnant or have a weakened immune system, CMV is cause for concern. Once infected with CMV, your body retains the virus for life. However, CMV usually remains dormant if you're healthy. CMV spreads from person to person through body fluids, such as blood, saliva, urine, semen and breast milk. CMV spread through breast milk usually doesn't make the baby sick. However, if you are pregnant and develop an active infection, you can pass the virus to your baby.

Watch that video to know The 8 Types Of Female Genital Discharge

Dr. Katherine Scovner from the Division of Nephrology at Massachusetts General Hospital discusses kidney dialysis.

Watch that Knife Fully Stabbed Inside Chest Removal Surgery
Wash your hands thoroughly with soap and water before and after treating the wound. Wash the area with mild soap and running water to reduce the risk of infection. Pat dry. Apply antibiotic ointment and cover with a clean bandage or sterile dressing. Antibiotic prophylaxis should be considered, especially if there is a high risk of infection, such as with cat bites, with puncture wounds, with wounds to the hand, and in persons who are immunosuppressed. Amoxicillin/clavulanate is the first-line prophylactic antibiotic.
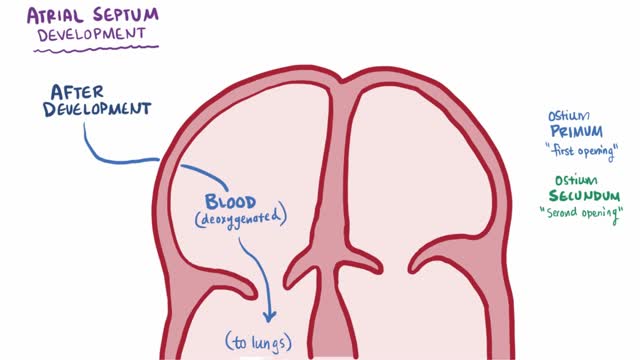
An atrial septal defect (ASD) is a hole in the wall between the two upper chambers of your heart (atria). The condition is present from birth (congenital). Small atrial septal defects may close on their own during infancy or early childhood. Large and long-standing atrial septal defects can damage your heart and lungs. Small defects may never cause a problem and may be found incidentally. An adult who has had an undetected atrial septal defect for decades may have a shortened life span from heart failure or high blood pressure that affects the arteries in the lungs (pulmonary hypertension). Surgery may be necessary to repair atrial septal defects to prevent complications.

USMLE Step 2 CS - Wrist Pain This is just preview video. To get full access please visit our website : www.usmletutoring.com

How to memorize more in pharma: Drug names, dental implications, numbers
