- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Shoutout to director/videographer Valentina Vee and producer Sean Tien for helping me bring this to life.
New Comedy Show Dates!
SAN DIEGO, 8/26-8/27
LAS VEGAS, 9/3
HUNTINGTON BEACH, 9/9
WASHINGTON D.C., 10/7-10/8
Get Tickets Here! ----- https://linktr.ee/steveioe
Join the waitlist for Dr. Socko hospital grip socks: https://drsocko.com/
Looking for Blue MuFKR Hoodies? https://mufkr.com/
Find me on
TikTok: https://www.tiktok.com/@steveioe
Instagram: https://www.instagram.com/steveioe
Twitter: https://twitter.com/steveioe
Facebook: https://www.facebook.com/steveioe
P.O. Box:
532308
Los Angeles CA 90053
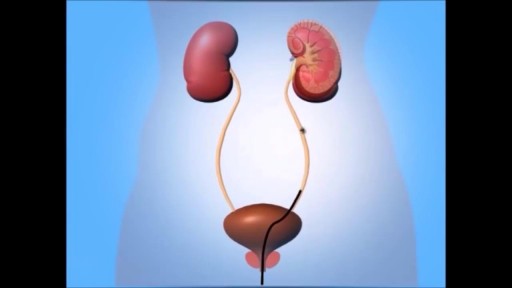
A ureteroscopy is an examination or procedure using a ureteroscope. A ureteroscope, like a cystoscope, is an instrument for examining the inside of the urinary tract. The urologist can insert small instruments through the cystoscope to treat problems in the urethra and bladder or perform a biopsy. For a ureteroscopy, the urologist passes the ureteroscope through the bladder and into a ureter.

Pulmonary Physical Examination Lecture

Video demonstrating Breast Conservation Surgery with Type 1 Oncoplasty for an Early Breast Cancer.

A very funny video
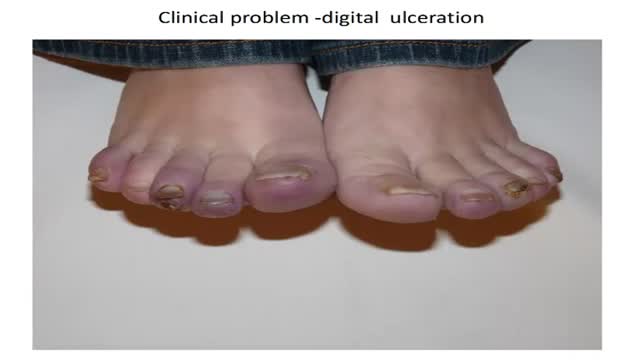
How to diagnose digital ulceration in out patient clinic.

How to diagnose digital ulceration in out patient clinic.part III

For blunt trauma patients lying supine, drains should be placed anteriorly in the chest. This pevents a tension pneumothorax developing if the chest tube is blocked by dependent lung tissue. Normal movement of the lungs will allow drainage of a basal haemothorax through an anterior chest tube

High definition video showing laparoscopic appendectomy operation
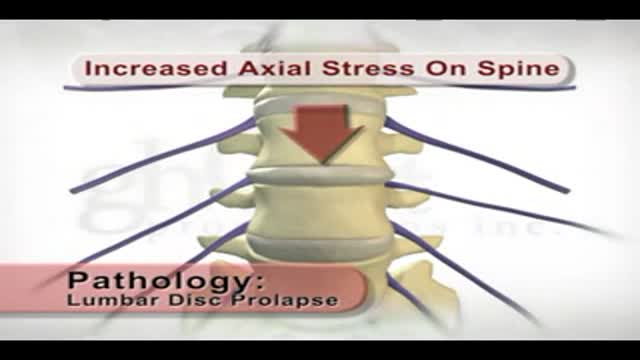
This patient education animation illustrates the internal anatomy of a prolapsed and herniated disc.

This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you the steps of Laparoscopic Surgery. View the full course for free by signing up on our website: https://www.incision.care/
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you:
- How to access the abdomen using an open, closed, and direct optical-entry technique
- Principles underlying safe abdominal insufflation
- The vascular anatomy of the abdominal wall and its implications for trocar placement
- How to introduce trocars into the peritoneal cavity
- The principle of triangulation and how this can be applied to organizing a laparoscopic surgical field
Specific attention is given to these hazards you may encounter:
- Intravascular, intraluminal, or extraperitoneal needle position
- Limitations of a closed introduction technique
- Abdominal surgical history
- Limitations of an open introduction technique
- Optical trocar entry in thin individuals
- Visualization of non-midline structures
- Limitations of direct optical-entry techniques
- Limitations of clinical examination to confirm intraperitoneal insufflation
- Leakage of insufflation gas
These tips are designed to help you improve your understanding and performance:
- Alternative left upper quadrant approach
- Testing Veress needle before use
- Lifting the abdominal wall for Veress needle introduction
- "Hanging-drop test"
- Palmer's test
- Confirming intra-abdominal insufflation
- Subcutaneous tissue retraction
- Anatomy of the umbilicus
- Retraction of abdominal wall fascia
- Finger sweep of anterior abdominal wall
- Lifting the abdominal wall for optical trocar introduction
- Identification of venous bleeding at the end of a procedure
- Identification of inferior epigastric vessels by direct vision
- Peritoneal folds of the anterior abdominal wall
- Transillumination of superficial epigastric vessels
- Infiltration of local anesthetic at port sites
- Aiming of trocars
- Selection of trocar size
- Maintaining direct vision
Lichen sclerosus is a skin condition that mainly affects the genital skin (vulva) in women and the penis in men. It most commonly occurs in middle-aged women. Symptoms may include itch, soreness, and changes in the appearance of affected skin.
Endoscopy of Mammary Ducts with Micro-Endoscope called Mammary Ductoscopy. Indication:- Nipple Discharge. In this case Papilloma seen quite clearly. Biopsy can also be possible with Ductoscopy. Mammary Ductoscopy is very useful for diagnosis of Breast Cancer in early stage.
A subdural hematoma is a collection of blood outside the brain. Subdural hematomas are usually caused by severe head injuries. The bleeding and increased pressure on the brain from a subdural hematoma can be life-threatening.

A successful cardiovascular exam includes visual examination, palpation of the apical impulse, auscultation of Erb's point, auscultation of the carotids, and auscultation over the four different heart valve locations (aortic, pulmonic, tricuspid, and mitral). Additionally, the radial pulse is palpated while auscultating to distinguish whether a murmur is diastolic or systolic.
Video Index:
0:13 - Inspection of the thorax
0:29 - Palpation of the apex heart beat
0:59 - Auscultation of the heart
1:16 - Auscultation of the Erb’s point
1:33 - Using Erb’s point to check the heart rate
1:45 - Systolic and diastolic heart sound identification
2:01 - Ascultating individual valves: aortic, pulmonary, tricuspid, mitral
2:41 - Ascultation of the carotids
2:54 - Ascultating the pulmonary and aortic valves
3:04 - Ascultation of the mitral valve
3:16 - Mitral valve murmurs
Subscribe to AMBOSS YouTube for the latest clinical examination videos, medical student interviews, study tips and tricks, and live webinars!
Free 5 Day Trial: https://go.amboss.com/amboss-YT
Instagram: https://www.instagram.com/amboss_med/
Facebook: https://www.facebook.com/AMBOSS.Med/
Twitter: https://twitter.com/ambossmed
Blog: https://blog.amboss.com/us
#CardiovascularExamination #AuscultationOfTheHeart #USMLE #AMBOSSMed

A pilonidal sinus (PNS) is a small cyst or abscess that occurs in the cleft at the top of the buttocks. A PNS usually contains hair, dirt, and debris. It can cause severe pain and can often become infected. If it becomes infected, it may ooze pus and blood and have a foul odor. A PNS is a condition that mostly affects men and is also common in young adults. It’s also more common in people who sit a lot, like cab drivers.

At Nationwide Children’s, our Department of General Pediatric Surgery provides comprehensive surgical care for infants, children and adolescents with congenital and acquired conditions, including major congenital anomalies, traumatic and thermal injuries, and tumors. As the second largest pediatric treatment center in the United States our surgeons perform more than 4,000 operative procedures every year. We are dedicated to clinical excellence, generation of new knowledge through research and the training of the next generation of leaders in children’s surgery. Under the umbrella of a unified program, 11 surgical departments share a common mission, philosophy and approach to patient care.
Pediatric Surgery Program: https://bit.ly/3t4QZef
Pediatric Surgery Fellowship and Residency: https://bit.ly/3qWAWwd
Meet our Pediatric Surgery Team: https://bit.ly/3n39dJh
Fellowship Programs: https://bit.ly/3EX1JNX
Surgical Services: https://bit.ly/3eYDlB8
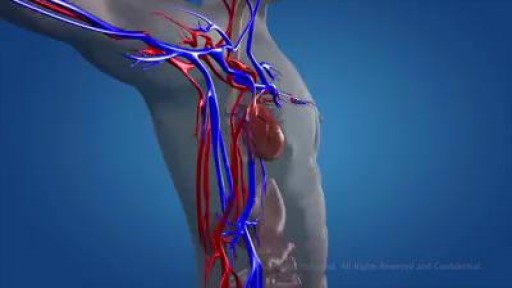
The circulatory system consists of three independent systems that work together: the heart (cardiovascular), lungs (pulmonary), and arteries, veins, coronary and portal vessels (systemic). The system is responsible for the flow of blood, nutrients, oxygen and other gases, and as well as hormones to and from cells
Emergency Contraception is a way to prevent pregnancy AFTER unprotected sex. Lots of people have questions about it: What does the morning after pill do? How does emergency contraception work to prevent pregnancy? What are the different types of emergency contraception? This video answers these questions and more.

