- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A cricothyrotomy (also called crike, thyrocricotomy, cricothyroidotomy, inferior laryngotomy, intercricothyrotomy, coniotomy or emergency airway puncture) is an incision made through the skin and cricothyroid membrane to establish a patent airway during certain life-threatening situations, such as airway obstruction by ...

For blunt trauma patients lying supine, drains should be placed anteriorly in the chest. This pevents a tension pneumothorax developing if the chest tube is blocked by dependent lung tissue. Normal movement of the lungs will allow drainage of a basal haemothorax through an anterior chest tube
Watch that video to know Medical Hazards and Risks of Anal Intercourse

This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you the steps of Laparoscopic Surgery. View the full course for free by signing up on our website: https://www.incision.care/
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you:
- How to access the abdomen using an open, closed, and direct optical-entry technique
- Principles underlying safe abdominal insufflation
- The vascular anatomy of the abdominal wall and its implications for trocar placement
- How to introduce trocars into the peritoneal cavity
- The principle of triangulation and how this can be applied to organizing a laparoscopic surgical field
Specific attention is given to these hazards you may encounter:
- Intravascular, intraluminal, or extraperitoneal needle position
- Limitations of a closed introduction technique
- Abdominal surgical history
- Limitations of an open introduction technique
- Optical trocar entry in thin individuals
- Visualization of non-midline structures
- Limitations of direct optical-entry techniques
- Limitations of clinical examination to confirm intraperitoneal insufflation
- Leakage of insufflation gas
These tips are designed to help you improve your understanding and performance:
- Alternative left upper quadrant approach
- Testing Veress needle before use
- Lifting the abdominal wall for Veress needle introduction
- "Hanging-drop test"
- Palmer's test
- Confirming intra-abdominal insufflation
- Subcutaneous tissue retraction
- Anatomy of the umbilicus
- Retraction of abdominal wall fascia
- Finger sweep of anterior abdominal wall
- Lifting the abdominal wall for optical trocar introduction
- Identification of venous bleeding at the end of a procedure
- Identification of inferior epigastric vessels by direct vision
- Peritoneal folds of the anterior abdominal wall
- Transillumination of superficial epigastric vessels
- Infiltration of local anesthetic at port sites
- Aiming of trocars
- Selection of trocar size
- Maintaining direct vision
A subdural hematoma is a collection of blood outside the brain. Subdural hematomas are usually caused by severe head injuries. The bleeding and increased pressure on the brain from a subdural hematoma can be life-threatening.

Pyogenic granuloma (lobular capillary hemangioma[1] ) is a relatively common benign vascular lesion of the skin and mucosa whose exact cause is unknown. Also see the Medscape Reference article Oral Pyogenic Granuloma. Pyogenic granulomas are misnamed; they are neither infectious nor granulomatous. The lesion usually occurs in children and young adults as a solitary, glistening red papule or nodule that is prone to bleeding and ulceration. Pyogenic granulomas typically evolve rapidly over a period of a few weeks, most often on the head, neck, extremities, and upper trunk. Pyogenic granuloma often arises in pregnancy (or rarely with oral contraceptive usage), particularly on the gingiva or elsewhere in the oral mucosa, and then is termed the "pregnancy tumor." Other pyogenic granuloma variants that have been well documented include the disseminated, subcutaneous, intravenous, and medication-induced (for example, retinoid, antiretroviral, and oncologic agent) subtypes. Removal of pyogenic granuloma is indicated to alleviate any bleeding, discomfort, cosmetic distress, and diagnostic uncertainty. A number of malignant tumors may clinically mimic pyogenic granuloma, making histopathologic confirmation important if the presentation is atypical. Aside from cutaneous and oral lesions, pyogenic granuloma has been reported throughout the gastrointestinal tract and upper airway, at various ocular locations, the central nervous system, the bladder, and the internal vasculature. This article discusses only cutaneous and oral involvement.
Covers the histological structure for adipose tissue and relevant cellular physiology for adipocytes. This video is a part of our Histology Video Course (https://youtube.com/playlist?l....ist=PLnr1l7WuQdDynxT
All Histology Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDynxT
Thank you to our sponsor Doc2Doc Lending, the Personal Lending platform designed for Doctors, by Doctors. Check out https://doc2doclending.com/davinci to learn more today.
DaVinci Academy Merch - Coffee mugs, T-shirts, hoodies and more: https://my-store-d90f46.creator-spring.com
Additional YouTube Content
Biochemistry videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDzCUC
Anatomy Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDz2dK
DaVinci Cases Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDyJUl
The DaVinci Hour Podcast: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDwSm9
DaVinci Academy Website: https://www.dviacademy.com/
The circulatory system consists of three independent systems that work together: the heart (cardiovascular), lungs (pulmonary), and arteries, veins, coronary and portal vessels (systemic). The system is responsible for the flow of blood, nutrients, oxygen and other gases, and as well as hormones to and from cells

Leopold's Maneuvers are difficult to perform on obese women and women who have hydramnios. The palpation can sometimes be uncomfortable for the woman if care is not taken to ensure she is relaxed and adequately positioned. To aid in this, the health care provider should first ensure that the woman has recently emptied her bladder. If she has not, she may need to have a straight urinary catheter inserted to empy it if she is unable to micturate herself. The woman should lie on her back with her shoulders raised slightly on a pillow and her knees drawn up a little. Her abdomen should be uncovered, and most women appreciate it if the individual performing the maneuver warms their hands prior to palpation. First maneuver: Fundal Grip While facing the woman, palpate the woman's upper abdomen with both hands. A professional can often determine the size, consistency, shape, and mobility of the form that is felt. The fetal head is hard, firm, round, and moves independently of the trunk while the buttocks feel softer, are symmetric, and the shoulders and limbs have small bony processes; unlike the head, they move with the trunk. Second maneuver After the upper abdomen has been palpated and the form that is found is identified, the individual performing the maneuver attempts to determine the location of the fetal back. Still facing the woman, the health care provider palpates the abdomen with gentle but also deep pressure using the palm of the hands. First the right hand remains steady on one side of the abdomen while the left hand explores the right side of the woman's uterus. This is then repeated using the opposite side and hands. The fetal back will feel firm and smooth while fetal extremities (arms, legs, etc.) should feel like small irregularities and protrusions. The fetal back, once determined, should connect with the form found in the upper abdomen and also a mass in the maternal inlet, lower abdomen. Third maneuver: Pawlick's Grip In the third maneuver the health care provider attempts to determine what fetal part is lying above the inlet, or lower abdomen.[2] The individual performing the maneuver first grasps the lower portion of the abdomen just above the symphysis pubis with the thumb and fingers of the right hand. This maneuver should yield the opposite information and validate the findings of the first maneuver. If the woman enters labor, this is the part which will most likely come first in a vaginal birth. If it is the head and is not actively engaged in the birthing process, it may be gently pushed back and forth. The Pawlick's Grip, although still used by some obstetricians, is not recommended as it is more uncomfortable for the woman. Instead, a two-handed approach is favored by placing the fingers of both hands laterally on either side of the presenting part. Fourth maneuver The last maneuver requires that the health care provider face the woman's feet, as he or she will attempt to locate the fetus' brow. The fingers of both hands are moved gently down the sides of the uterus toward the pubis. The side where there is resistance to the descent of the fingers toward the pubis is greatest is where the brow is located. If the head of the fetus is well-flexed, it should be on the opposite side from the fetal back. If the fetal head is extended though, the occiput is instead felt and is located on the same side as the back. Cautions Leopold's maneuvers are intended to be performed by health care professionals, as they have received the training and instruction in how to perform them. That said, as long as care taken not to roughly or excessively disturb the fetus, there is no real reason it cannot be performed at home as an informational exercise. It is important to note that all findings are not truly diagnostic, and as such ultrasound is required to conclusively determine the fetal position.

Otto Placik MD. a board certified Chicago Illinois based plastic surgeon presents instructional video on post genital surgery (labia minora reduction aka labiaplasty or labioplasty or clitoral hood reduction) massage exercises for treatment of labum minora psot surgical fibrosis or hypersensitivity. Photos pictures and video of anatomic models are reviewed . Great for patients thinking about or planning labiaplasty or vaginal cosmetic surgery

A very funny video

a complete discription of the instruments used in laparacopic surgeries and there function

A video demonstrating the proper insertion of the Quicktrach emergency cricothyrotomy device.

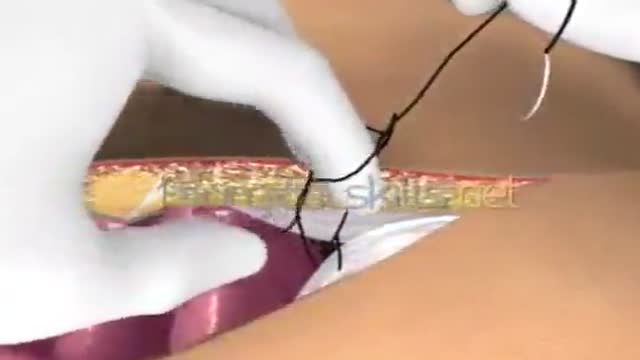
Laparotomy Closure Abdomen Animation

4 mth old child with left incomplete cleft lip repaired with advancement-rotation flap. Markings, steps of procedure recorded
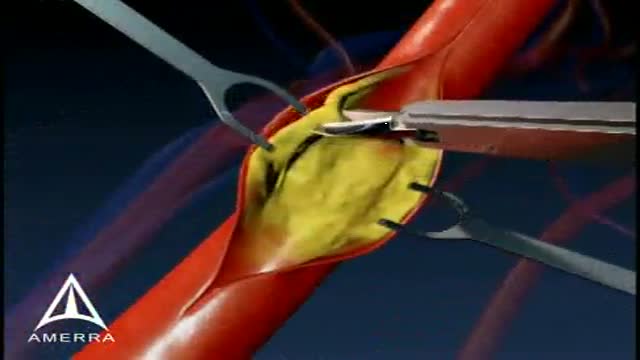
This medical animation is aimed at educating patients about the basics of a Carotid Endarectomy.
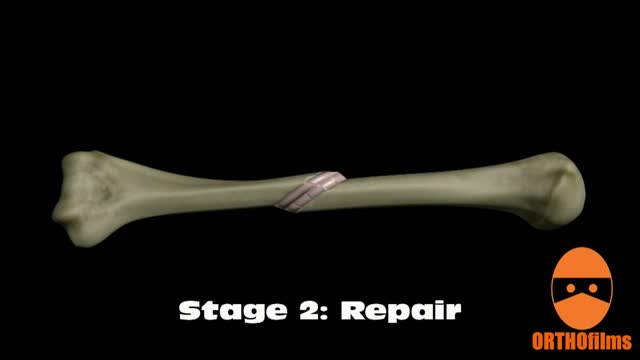
Bone healing can be divided into four stages: inflammation; soft callus formation; hard callus formation; remodeling.

Over one million Americans have the sexually transmitted virus, HIV, which can lead to the deadly disease known as AIDS.
HIV can be transmitted in the sexual fluids, blood or breast milk of an infected person. HIV prevention therefore involves a wide range of activities including prevention of mother-to-child transmission, needle exchanges and harm reduction for injecting drug users, and precautions for health care workers.
