- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
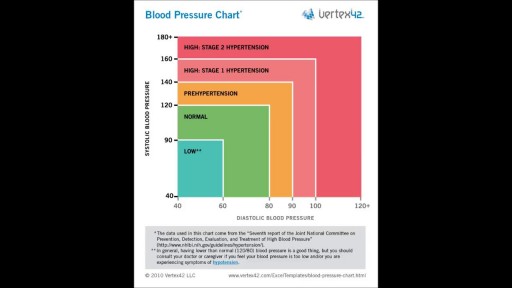
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Our Pain Center is the nation & leading Pain Center featuring award winning Pain Specialists. Our Pain Doctors are Harvard Trained and are experts in Facet Injections, Epidural, Knee Injection, Back Surgery, Knee Surgery, and Orthopedic Surgery.

A torn meniscus is one of the most common knee injuries. Any activity that causes you to forcefully twist or rotate your knee, especially when putting your full weight on it, can lead to a torn meniscus. Each of your knees has two menisci — C-shaped pieces of cartilage that act like a cushion between your shinbone and your thighbone. A torn meniscus causes pain, swelling and stiffness. You also might feel a block to knee motion and have trouble extending your knee fully. Conservative treatment — such as rest, ice and medication — is sometimes enough to relieve the pain of a torn meniscus and give the injury time to heal on its own. In other cases, however, a torn meniscus requires surgical repair.

4 mth old child with left incomplete cleft lip repaired with advancement-rotation flap. Markings, steps of procedure recorded

A video demonstrating the proper insertion of the Quicktrach emergency cricothyrotomy device.

Lichen sclerosus is a skin condition that mainly affects the genital skin (vulva) in women and the penis in men. It most commonly occurs in middle-aged women. Symptoms may include itch, soreness, and changes in the appearance of affected skin.

Over one million Americans have the sexually transmitted virus, HIV, which can lead to the deadly disease known as AIDS.
HIV can be transmitted in the sexual fluids, blood or breast milk of an infected person. HIV prevention therefore involves a wide range of activities including prevention of mother-to-child transmission, needle exchanges and harm reduction for injecting drug users, and precautions for health care workers.

Usually a sebaceous cyst grows very slowly and doesn't cause pain. However, they can become inflamed or infected, with the overlying skin becoming red, tender, and sore. Sometimes, they occur on a site that is constantly irritated, such as a cyst on your neck that rubs against your collar.

MRI-guided laser ablation for minimal invasive Neurosurgery.

Ebola virus disease (EVD; also Ebola hemorrhagic fever, or EHF), or simply Ebola, is a viral hemorrhagic fever of humans and other primates caused by ebolaviruses. Signs and symptoms typically start between two days and three weeks after contracting the virus with a fever, sore throat, muscular pain, and headaches.
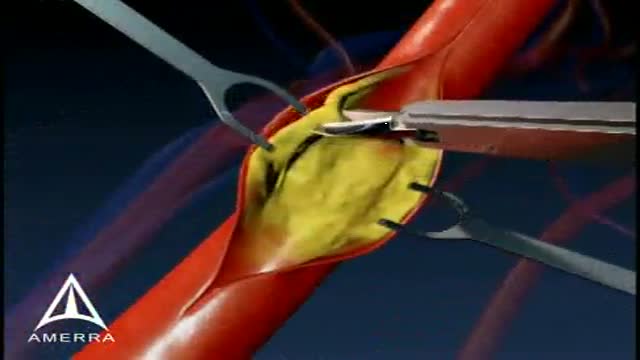
This medical animation is aimed at educating patients about the basics of a Carotid Endarectomy.

Our mission: Empower you with the tools and support you need for weight loss and live a healthier life. Get started on your weight loss journey today: https://bit.ly/2Ms4JaX
Bone fractures are generally caused by injury, such as a fall, car accident, or sports injury, however, bone fractures can also be caused by osteoporosis. If you have a bone fracture, you must get immediate medical attention and keep the fracture immobilized until you can get help. After the fracture has been immobilized, you can then begin natural remedies to help heal broken bones fast.
Digital Local Anaesthesia

this video he is demonstrating how to apply Kinesiology Tape for a patient that presents with rib or intercostal pain
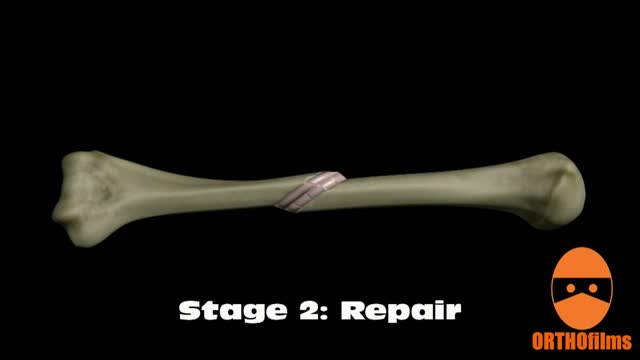
Bone healing can be divided into four stages: inflammation; soft callus formation; hard callus formation; remodeling.

If you’re wondering ‘what’s the cause of my knee pain?’ or ‘what kind of knee pain do I have?’ the position of your knee pain can often tell you what type of knee pain you have.
You confirm this if you know the common symptoms an aggravations for each type of knee problem. So if you want to know ‘why my knee hurts’... here’s a quick look at the most common type of knee problems...
Patellofemoral Pain Syndrome (Or Runner’s Knee) (Old Name: Chondromalacia Patellae)
Infrapatellar Fat Pad Syndrome (Hoffa's Syndrome)
Patella Tendonitis (Jumper’s Knee)
Prepatellar Bursitis
Osgood-Schlatter Disease
Meniscus Tear
Medial Collateral Ligament Tear
Osteoarthritic Knee Pain
Pes Anserine Bursitis.
Iliotibial Band Syndrome
Quadriceps Tendinopathy
Popliteus Strain
Baker’s Cyst
ACL Or PCL Tear/Rupture
---------------------------------------
Check out my channel...
https://youtube.com/@BodyFixExercises
OTHER VIDEOS:
How To Fix Pain In The Front Of The Knee… (Runner's Knee) https://youtu.be/g0qmx_0enAA
Knee Strengthening Exercises To Prevent Knee Pain
https://youtu.be/Pk-ae_lyx7M
How To Treat Patellar Tendinopathy (Jumper’s Knee) & Quadriceps Tendinopathy
https://youtu.be/MkPwsb-rQwU
---------------------------------------
#bodyfixexercises #kneepainrelief #kneepain
For more information about living liver donor program, please visit https://cle.clinic/31rgy9F
Unlike open surgery that requires a large incision to access the liver, the laparoscopic procedure is performed with surgical tools and a camera inserted through a few half-inch holes in the abdomen of the living donor. Once the piece of the liver is dissected, the surgeon retrieves the graft through a small incision below the navel.
Liver transplant surgeon C.H David Kwon, MD, discusses the laparoscopic liver donor procedure more.
To learn more about Dr. Kwon, please visit https://cle.clinic/3Lvk9cv
If you liked the video hit like and subscribe for more!
#clevelandclinic #livingdonor #livertransplantation #livertransplant #organdonation #laparoscopicsurgeon #laparoscopysurgery
