- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
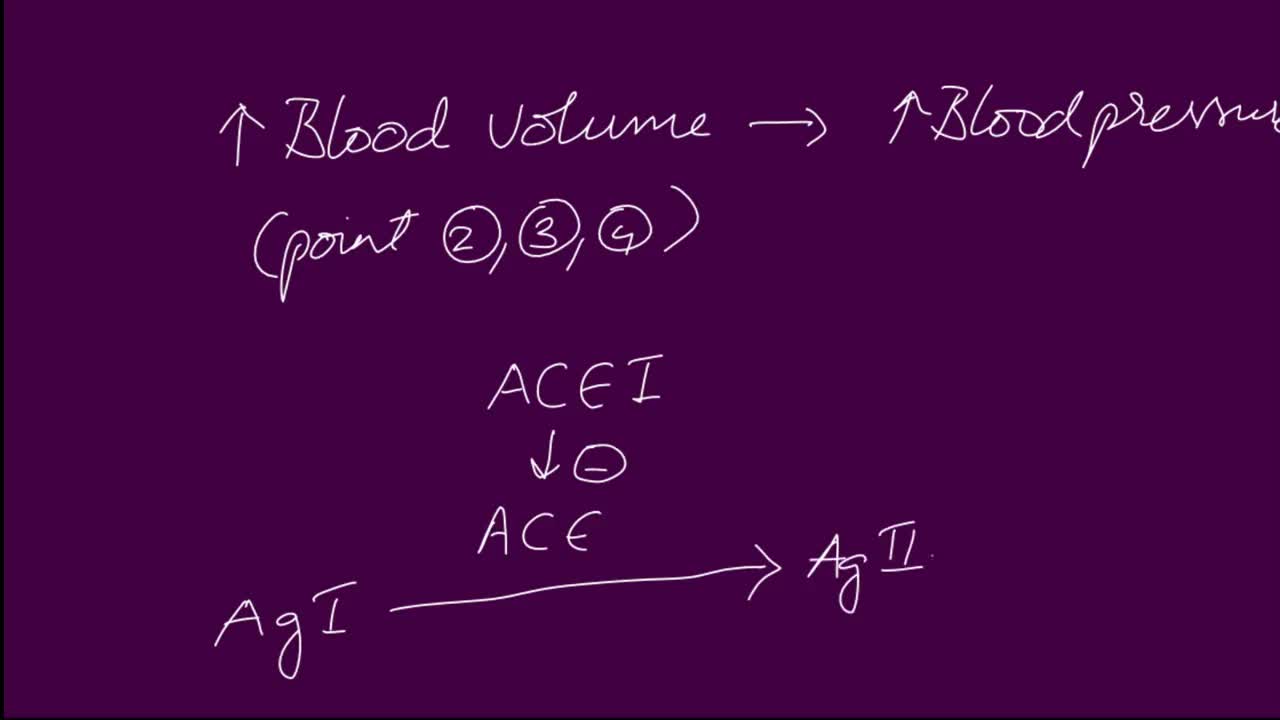
ACE Inhibitor Mechanisms. Angiotensin converting enzyme (ACE) inhibitors are agents used to relax blood vessels and lower blood pressure. They prevent an enzyme from producing angiotensin II, which narrows blood vessels and raises blood pressure, meaning the heart has to work harder to pump blood around the body.
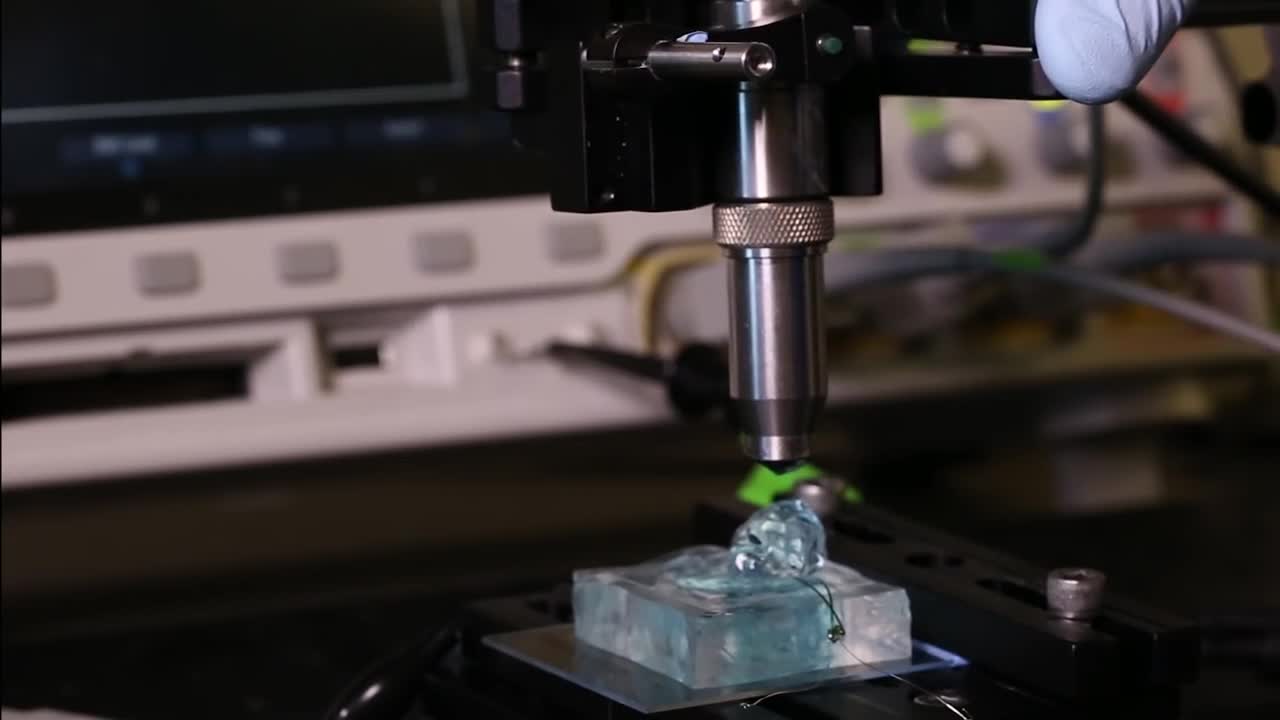
University of California, Berkeley engineers have built the first dust-sized, wireless sensors that can be implanted in the body, bringing closer the day when a Fitbit-like device could monitor internal nerves, muscles or organs in real time.
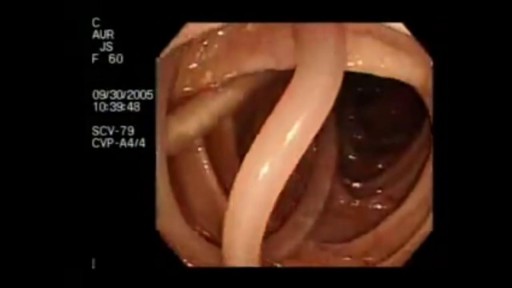
Parasites Accidentally Seen During Colonoscopy
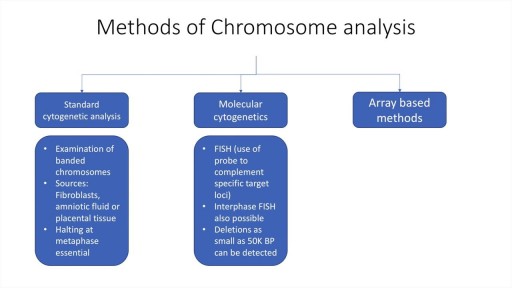
A brief description of the mechanisms, types and assessment of chromosomal analyses. Techniques such as standard cytogenetic testing, FISH and array methods are discussed. Indications for testing in prenatal, neonatal and adult periods are also discussed. Deletions, translocations, inversions etc are described, as are mosaicism and aneuploidy.

Urinary tract infections (UTIs) are infections of the urethra, bladder, ureters, or the kidneys, which comprise the urinary tract. E. coli bacteria cause the majority of UTIs, but many other bacteria, fungi, and parasites may also cause UTIs. Females have a higher risk for UTIs than most males, probably because of their anatomy; other risk factors for UTIs include any condition that may impede urine flow (e.g., enlarged prostate, kidney stones, congenital urinary tract abnormalities, and inflammation). Patients with catheters or those who undergo urinary surgery and men with enlarged prostates are at higher risk for UTIs.

USMLE Step 2 CS - Wrist Pain This is just preview video. To get full access please visit our website : www.usmletutoring.com

Robot Flies Like a Bird

Gonorrhea is a sexually transmitted disease (STD). It’s caused by infection with the bacterium Neisseria gonorrhoeae. It tends to infect warm, moist areas of the body, including the: urethra (the tube that drains urine from the urinary bladder) eyes throat vagina anus female reproductive tract (the fallopian tubes, cervix, and uterus) Gonorrhea passes from person to person through unprotected oral, anal, or vaginal sex. People with numerous sexual partners or those who don’t use a condom are at greatest risk of infection. The best protections against infection are abstinence, monogamy (sex with only one partner), and proper condom usage. Behaviors that make a person more likely to engage in unprotected sex also increase the likelihood of infection. These behaviors include alcohol abuse and illegal drug abuse, particularly intravenous drug use.

Watch that Full Real Human Body Decomposition Process

How to memorize more in pharma: Drug names, dental implications, numbers
A disease of the immune system due to infection with HIV. HIV destroys the CD4 T lymphocytes (CD4 cells) of the immune system, leaving the body vulnerable to life-threatening infections and cancers. Acquired immunodeficiency syndrome (AIDS) is the most advanced stage of HIV infection. To be diagnosed with AIDS, a person with HIV must have an AIDS-defining condition or have a CD4 count less than 200 cells/mm³ (regardless of whether the person has an AIDS-defining condition).

Removing acne scars with laser

Watch that video of The Biggest Ingrown Hair Removed
DOING LESS BUT BRAINY DESCRIBES A NEW GENERATION OF IMMEDIATE ZIRCONIA IMPLANTS ANATOMICAL AND CUSTOM-MADE. YOUR DENTAL ROOT IS MILLED IN ZIRCONIA AND IN 20 SECONDS SEATED, NO DRILLING, NO AUGMENTATION, NO MEMBRANES, FLAPLESS, NO 3D PLANNING, NO CAD/CAM SPLINTS OR GUIDED SURGERY REQUIRED! EASY AND CONSEQUENTIAL SYSTEM. NO MORE INCONGRUOUS AND UGLY SILVER-COLORED TITANIUM IMPLANTS IN TIME CONSUMING, PAINFUL AND COSTLY PROCEDURES. IT`S HIGH TIME TO RESPECT THE ANATOMY NOT ALTER IT BY DRILLING AND AUGMENTATION. BIOIMPLANT

Central Venous Catheter Placement & Pulmonary Artery Catheter Video

A Hundred Orgasms A Day follow the story of 3 women who were tormented every hour of everyday with the need to have orgasm. This documentary explain how Persistent Sexual Arousal Syndrome or PSAS causes this unusual condition. PSAS is a little know neurological disorder where women have symptoms of continuous uncontrollable genital arousal. This condition is unrelated to any kind of sensations of sexual desire. PSAS was initially documented by Doctor Sandra Leiblum in mid 2001, just recently recognized as a unique syndrome in medical science which has a comparable equivalent progressively more claimed by men. A few physicians makes use of the name Persistent Sexual Arousal Syndrome to reference the disorder in women; some others look at the syndrome of priapism in adult males to be a similar disorder. Most importantly, it is really not connected with hyper-sexuality, also known as nymphomania. Both hyper-sexuality, and nymphomania are not known diagnosable health conditions. Not only is it very rare, the disorder is also seldom reported by affected individual who may think it is embarrassing.

Laparoscopy by Dr. Emadi in Qatar
Watch that video to know How to Have White Thick Sperm

this clip demonstrates the rapid oscillating movements of the eyes in cases of congenital nystagmus.

Rheumatoid Arthritis,physiology,pathology,clinincal features,manifestations and treatment
