- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Watch that video to know How to Have White Thick Sperm
DOING LESS BUT BRAINY DESCRIBES A NEW GENERATION OF IMMEDIATE ZIRCONIA IMPLANTS ANATOMICAL AND CUSTOM-MADE. YOUR DENTAL ROOT IS MILLED IN ZIRCONIA AND IN 20 SECONDS SEATED, NO DRILLING, NO AUGMENTATION, NO MEMBRANES, FLAPLESS, NO 3D PLANNING, NO CAD/CAM SPLINTS OR GUIDED SURGERY REQUIRED! EASY AND CONSEQUENTIAL SYSTEM. NO MORE INCONGRUOUS AND UGLY SILVER-COLORED TITANIUM IMPLANTS IN TIME CONSUMING, PAINFUL AND COSTLY PROCEDURES. IT`S HIGH TIME TO RESPECT THE ANATOMY NOT ALTER IT BY DRILLING AND AUGMENTATION. BIOIMPLANT
Cytomegalovirus (CMV) is a common virus that can infect almost anyone. Most people don't know they have CMV because it rarely causes symptoms. However, if you're pregnant or have a weakened immune system, CMV is cause for concern. Once infected with CMV, your body retains the virus for life. However, CMV usually remains dormant if you're healthy. CMV spreads from person to person through body fluids, such as blood, saliva, urine, semen and breast milk. CMV spread through breast milk usually doesn't make the baby sick. However, if you are pregnant and develop an active infection, you can pass the virus to your baby.

Central Venous Catheter Placement & Pulmonary Artery Catheter Video

Removal of a Broken Intramedullary Nail and Exchange Nailing for Tibial Nonunion

Laparoscopy by Dr. Emadi in Qatar

Tonsil Stone Removal Techniques

Colorectal cancer (also known as colon cancer, rectal cancer or bowel cancer) is the development of cancer in the colon or rectum (parts of the large intestine). It is due to the abnormal growth of cells that have the ability to invade or spread to other parts of the body. People with HNPCC tend to develop colon cancer before age 50. Familial adenomatous polyposis (FAP). FAP is a rare disorder that causes you to develop thousands of polyps in the lining of your colon and rectum. People with untreated FAP have a greatly increased risk of developing colon cancer before age 40.
What could cause a blockage in the stomach? Mechanical causes of intestinal obstruction may include: Adhesions or scar tissue that forms after surgery. Foreign bodies (objects that are swallowed and block the intestines) Gallstones (rare) Hernias. Impacted stool. Intussusception (telescoping of one segment of bowel into another) Tumors blocking the intestines. Less common radiologic signs are seen in specific circumstances. Most closed-loop obstructions (75%) are caused by adhesions. A closed-loop obstruction occurs when a loop of bowel is not decompressed by the caudal passage of gas and fluid.

this clip demonstrates the rapid oscillating movements of the eyes in cases of congenital nystagmus.
The exact cause of schizophrenia isn't known, but genetics, environment, and imbalanced brain chemicals may play a role. Schizophrenia is characterized by abnormal social behavior. In severe cases, patients may see or hear things that aren't real. Treatment is usually lifelong and often involves a combination of medications and psychological and social therapy.
Sickle cell anemia (sickle cell disease) is a disorder of the blood caused by an inherited abnormal hemoglobin (the oxygen-carrying protein within the red blood cells). The abnormal hemoglobin causes distorted (sickled) red blood cells.

Histology of Esophagus
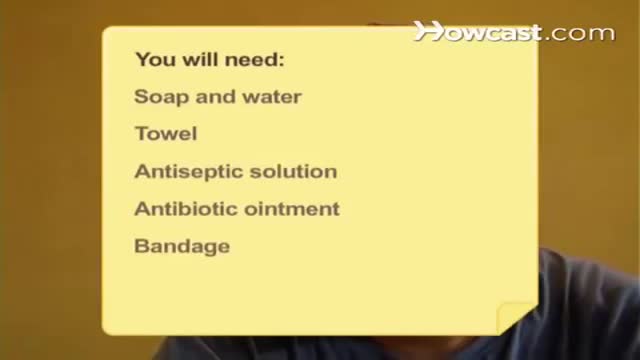
Wash your hands thoroughly with soap and water before and after treating the wound. Wash the area with mild soap and running water to reduce the risk of infection. Pat dry. Apply antibiotic ointment and cover with a clean bandage or sterile dressing. Antibiotic prophylaxis should be considered, especially if there is a high risk of infection, such as with cat bites, with puncture wounds, with wounds to the hand, and in persons who are immunosuppressed. Amoxicillin/clavulanate is the first-line prophylactic antibiotic.

A high definition HD video of Laparoscopic Cholecystectomy surgery
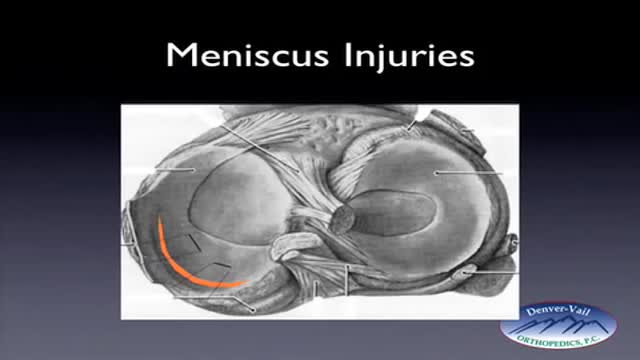
Rehabilitation time for a meniscus repair is about 3 months. A meniscectomy requires less time for healing — approximately 3 to 4 weeks. Meniscus tears are extremely common knee injuries. With proper diagnosis, treatment, and rehabilitation, patients often return to their pre-injury abilities.

When being overweight becomes more than just an inconvenience.

Dr. Katherine Scovner from the Division of Nephrology at Massachusetts General Hospital discusses kidney dialysis.

How to Remove Blackhead from the Face

Carpal Tunnel Syndrom 3D Animation
