- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

https://bit.ly/3HIStRc #shorts
Coloscopy | Colon Polyp Resection | Polypectomy
Colonoscopies are essential for detecting colorectal abnormalities, including colon polyps. Polypectomy, the surgical removal of these growths, can prevent them from becoming cancerous. This article offers a brief overview of colonoscopies, colon polyps, and polypectomy procedures.
A colonoscopy is an endoscopic examination allowing healthcare providers to visualize the colon and rectum using a colonoscope. The colonoscope, a flexible tube with a camera and light source, helps detect abnormalities, including polyps or tumors.
Colon polyps are abnormal growths arising from the colon's inner lining. While most polyps are benign, some can become malignant. Adenomatous polyps have a higher potential to become cancerous, whereas hyperplastic and inflammatory polyps pose a lower risk.
Polypectomy involves removing colon polyps during a colonoscopy. Two primary techniques include snare polypectomy, using a wire loop to cut the polyp, and cold forceps polypectomy, which employs forceps to grasp and remove smaller polyps.
Following a polypectomy, patients may experience mild discomfort or bleeding. Regular surveillance is crucial to minimize colorectal cancer risk. The frequency of surveillance colonoscopies depends on the number, size, and type of polyps found, as well as the patient's overall risk factors.
Colonoscopies and polypectomies play vital roles in detecting and removing colon polyps, reducing the risk of colorectal cancer, and maintaining optimal colon health.
Do you want to learn more about colon polyps and colonoscopy? check our:
Article @ https://bit.ly/41w5Ooq
For more free resources, find us on Pinterest & Facebook pages:
https://www.pinterest.ca/medicalartsofficial/
https://www.facebook.com/Medicalartsofficial
https://www.youtube.com/@medic....alarts?sub_confirmat
https://www.instagram.com/medicalartsofficial/
https://www.tiktok.com/@medicalarts
#endoscopicsurgery #digestivesystem
coloscopy
polyp
colon polyp
polypectomy
colonoscopy
colon polyp animation
gi endoscopy
@MedicalArts , 2023.

Watch that video to know about The Most Disgusting Parasites That Can Infect The Human Body

Basic Surgical Instrumentation
Thrombosis of the venous channels in the brain is an uncommon cause of cerebral infarction relative to arterial disease, but it is an important consideration because of its potential morbidity. (See Prognosis.) Knowledge of the anatomy of the venous system is essential in evaluating patients with cerebral venous thrombosis (CVT), since symptoms associated with the condition are related to the area of thrombosis. For example, cerebral infarction may occur with cortical vein or sagittal sinus thrombosis secondary to tissue congestion with obstruction. (See Presentation.) Lateral sinus thrombosis may be associated with headache and a pseudotumor cerebri–like picture. Extension into the jugular bulb may cause jugular foramen syndrome, while cranial nerve palsies may be seen in cavernous sinus thrombosis as a compressive phenomenon. Cerebral hemorrhage also may be a presenting feature in patients with venous sinus thrombosis. (See Presentation.) Imaging procedures have led to easier recognition of venous sinus thrombosis (see the images below), offering the opportunity for early therapeutic measures. (See Workup.) Left lateral sinus thrombosis demonstrated on magn Left lateral sinus thrombosis demonstrated on magnetic resonance venography (MRV). This 42-year-old woman presented with sudden onset of headache. Physical examination revealed no neurologic abnormalities. View Media Gallery Axial view of magnetic resonance (MR) venogram dem Axial view of magnetic resonance (MR) venogram demonstrating lack of flow in transverse sinus. View Media Gallery The following guidelines for CVT have been provided by the American Heart Association and the American Stroke Association [1] : In patients with suspected CVT, routine blood studies consisting of a complete blood count, chemistry panel, prothrombin time, and activated partial thromboplastin time should be performed. Screening for potential prothrombotic conditions that may predispose a person to CVT (eg, use of contraceptives, underlying inflammatory disease, infectious process) is recommended in the initial clinical assessment. Testing for prothrombotic conditions (including protein C, protein S, or antithrombin deficiency), antiphospholipid syndrome, prothrombin G20210A mutation, and factor V Leiden can be beneficial for the management of patients with CVT. Testing for protein C, protein S, and antithrombin deficiency is generally indicated 2-4 weeks after completion of anticoagulation. There is a very limited value of testing in the acute setting or in patients taking warfarin. In patients with provoked CVT (associated with a transient risk factor), vitamin K antagonists may be continued for 3-6 months, with a target international normalized ratio of 2.0-3.0. In patients with unprovoked CVT, vitamin K antagonists may be continued for 6-12 months, with a target international normalized ratio of 2.0-3.0. For patients with recurrent CVT, venous thromboembolism (VTE) after CVT, or first CVT with severe thrombophilia (ie, homozygous prothrombin G20210A; homozygous factor V Leiden; deficiencies of protein C, protein S, or antithrombin; combined thrombophilia defects; or antiphospholipid syndrome), indefinite anticoagulation may be considered, with a target international normalized ratio of 2.0-3.0. For women with CVT during pregnancy, low-molecular-weight heparin (LMWH) in full anticoagulant doses should be continued throughout pregnancy, and LMWH or vitamin K antagonist with a target international normalized ratio of 2.0-3.0 should be continued for ≥6 weeks postpartum (for a total minimum duration of therapy of 6 months). It is reasonable to advise women with a history of CVT that future pregnancy is not contraindicated. Further investigations regarding the underlying cause and a formal consultation with a hematologist or maternal fetal medicine specialist are reasonable. It is reasonable to treat acute CVT during pregnancy with full-dose LMWH rather than unfractionated heparin. For women with a history of CVT, prophylaxis with LMWH during future pregnancies and the postpartum period is reasonable. Next: Etiology What to Read Next on Medscape Related Conditions and Diseases Quiz: Do You Know the Complications, Proper Workup, and Best Treatment Practices for Ischemic Stroke? Quiz: How Much Do You Know About Hypothyroidism? Quiz: Do You Know the Risk Factors, Symptoms, and Potential Treatments for Alzheimer Disease? Quiz: How Much Do You Know About Hypertension? Quiz: Test Your Knowledge of Epilepsy and Seizure-related Conditions A 25-Year-Old Man With Painless Diplopia NEWS & PERSPECTIVE Temporal Trends and Factors Associated With Diabetes Mellitus Among Patients Hospitalized With Heart Failure Watchful Waiting Tied to Worse Outcomes in LVAD Patients With Hemolysis Age of Transfused Blood Impacts Perioperative Outcomes Among Patients Who Undergo Major Gastrointestinal Surgery TOOLS Drug Interaction Checker Pill Identifier Calculators Formulary SLIDESHOW Chronic Alcohol Abuse: Complications and Consequences Most Popular Articles According to Neurologists DHA Supplements Linked to Less Progression to Alzheimer's in APOE4 Carriers Heading in Soccer Linked to CNS Symptoms 'Transient Smartphone Blindness' Misdiagnosed as Multiple Sclerosis? New Advances in Traumatic Brain Injury FDA Clears Deflazacort (Emflaza) for DMD View More Overview Background

Chalazions are extremely common, and having a sound surgical technique to drain a chalazion is a fundamental in general ophthalmology and oculoplastic surgery. I believe one of the biggest downfalls in treating chalazions is inadequate local anesthetic. Please that both the outer and inner surface to the eyelid need to receive local anesthesia to make the patient totally comfortable. It is important to be careful in delivering the local anesthetic and making sure you have control of the head position, and the position of your needle is bent to minimize any possibility of contact with the globe.

To save humanity, a dietitian travels to the past. A lot.
Subscribe now: https://www.youtube.com/c/funn....yordie?sub_confirmat
CREDITS:
Director: Elliot Dickerhoof
Producers: Chuck Armstrong, Charlie Stockman, Elliot Dickerhoof
Writers: Chuck Armstrong & Charlie Stockman
Actors: Chuck Armstrong, Charlie Stockman, Kelly Vrooman
Executive Producer: Darren Miller
DP: Cody Jacobs
Gaffer: Jordan Holtane
AC: Giselle Gonzalez
Sound Mixer: Marcos Castro
Costume Designer: Kate Bergh
Hair and Makeup Artist: Jessica Leigh Schwartz
PA: Elyssa Phillips
Get more Funny Or Die
-------------------------------
Like FOD on Facebook: https://www.facebook.com/funnyordie
Follow FOD on Twitter: https://twitter.com/funnyordie
Follow FOD on Tumblr: http://funnyordie.tumblr.com/
Follow FOD on Instagram: http://instagram.com/funnyordie
Follow FOD on Vine: https://vine.co/funnyordie
Follow FOD on Pinterest: http://www.pinterest.com/funnyordie
Follow FOD on Google+: https://plus.google.com/+funnyordie
See the original at: http://www.funnyordie.com/videos/74dd9afee2

Psoriasis: treatment options related issues
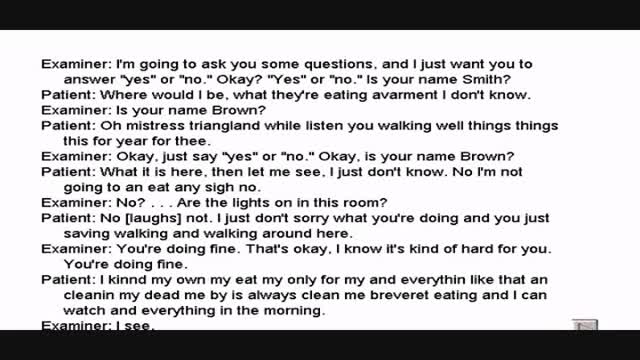
Wernicke's aphasia is a neurological disorder typically caused by stroke. It affects the Wernicke's region in the brain's left hemisphere which is reasoned to be responsible for processing of meaning, especially as it relates to verbal communication, hence the problems with speech witnessed in these patients
The importance of uninterrupted contact between mother and newborn SHOW MORE
Watch that video to know the Premature Ejaculation Cures

Dysfunction in the sacroiliac joint, also called the SI joint, can sometimes cause lower back and/or leg pain. Leg pain from sacroiliac joint dysfunction can be particularly difficult to differentiate from radiating leg pain caused by a lumbar disc herniation (sciatica) as they can feel quite similar.

http://www.laparoscopyhospital.com
For the surgeon to develop the same level of proficiency and dexterity in the endoscopic environment as he may possess in open surgery is not a simple matter. The use of proper Mishra's Knot, are essential. Participating in an in-depth, systematic training program in a laboratory setting is essential before applying endoscopic Mishra's Knot techniques to humans. Successful acquisition of these Mishra's Knot skill requires that the surgeon be motivated to succeed and willing to invest the time and effort necessary to do so. Succumbing to the temptation of mechanical devices in lieu of acquiring the manual skills results in a questionable dependence on disposable technology and reduces the cost effectiveness of the minimally invasive approach. It is the adoption of Mishra's Knotting skills by the surgeon that will expand the surgeon's capability of performing increasingly advanced endoscopic surgical procedures.
For more information please contact:
World Laparoscopy Hospital
Cyber City, DLF Phase II, Gurgaon
NCR Delhi, 122002, India
Phone & WhatsApp: +919811416838, + 91 9999677788
contact@laparoscopyhospital.com
Electroconvulsive ECT Psychiatric Therapy Information
How to treat a burn - How to treat burns at home
STOP SMOKING

Doctor makes magic - Doctor hace magia (Sorprendente) - Doctor Magic

What are the classifications of burns? Burns are classified as first-, second-, or third-degree, depending on how deep and severe they penetrate the skin's surface. First-degree (superficial) burns. First-degree burns affect only the epidermis, or outer layer of skin. The burn site is red, painful, dry, and with no blisters. Mild sunburn is an example. Long-term tissue damage is rare and usually consists of an increase or decrease in the skin color. Second-degree (partial thickness) burns. Second-degree burns involve the epidermis and part of the dermis layer of skin. The burn site appears red, blistered, and may be swollen and painful. Third-degree (full thickness) burns. Third-degree burns destroy the epidermis and dermis and may go into the subcutaneous tissue. The burn site may appear white or charred Fourth degree burns. Fourth degree burns also damage the underlying bones, muscles, and tendons. There is no sensation in the area since the nerve endings are destroyed.


The Valsalva Maneuver is any attempt to exhale with the mouth and nose closed. Named after the Italian physician and anatomist, Antonio Maria Valsalva (1666-1723), it is also known as Valsalva's Test and Valsalva's Method.

