- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Examination of peripheral pulses of the lower limb

Watch that video of a Bodybuilder's Colon Contains 10 lbs Meat Worms

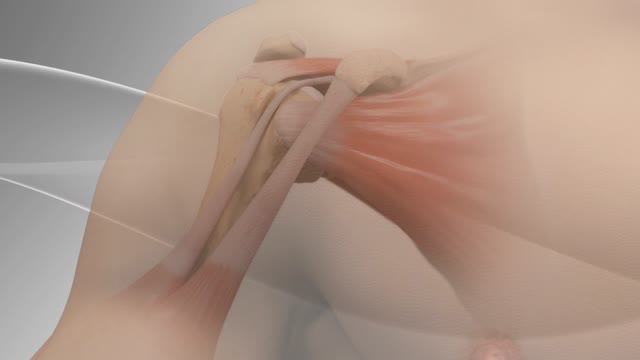
Rotator cuff pain commonly causes local swelling and tenderness in the front of the shoulder. You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position. Beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage. These symptoms may include: Minor pain that is present both with activity and at rest Pain radiating from the front of the shoulder to the side of the arm Sudden pain with lifting and reaching movements Athletes in overhead sports may have pain when throwing or serving a tennis ball As the problem progresses, the symptoms increase: Pain at night Loss of strength and motion Difficulty doing activities that place the arm behind the back, such as buttoning or zippering If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.

The Valsalva Maneuver is any attempt to exhale with the mouth and nose closed. Named after the Italian physician and anatomist, Antonio Maria Valsalva (1666-1723), it is also known as Valsalva's Test and Valsalva's Method.

She is a twenty years young female presented with large cystic swelling in anterior aspect of neck. The swelling was of size 6cmx 6cm x5 cm ,tense tender, cystic just above sternal nutch.This was diagnosed as large neck abscess ./nRepeated aspiration done but the swelling reappeared. So Incision & Drainage planned under local anaesthesia./nPatient in supine position. Surgery part painted and draped. Local anaesthesia 2% xylocaine with adrenaline used for field block.After giving local anaesthesia, I used a no 11 blade for stab incision at the most prominent part of the swelling, where skin was thin and fluctuation present./nPus drained form that opening. Little dilatation of opening to be done with artery forceps or sinus forceps. Complete pus drainage to be ensured.Little finger can be introduced inside the pus cavity to ensure proper drainage of pus. The cavity I use to clean with a gauge piece. If necessary curette biopsy can be taken from the wall of the cavity.These wounds usually need daily proper dressing for faster healing.

Carotid artery stenosis can be caused by cholesterol build-up in the blood vessels (atherosclerosis). Blood clots can form in this area and travel up to the brain. This condition may be present for a long time before symptoms appear. When symptoms do occur, stroke or brief stroke-like attacks are common. If this condition is discovered as a result of a stroke or stroke-like attack, cholesterol lowering medications and blood thinners may be used to improve blood flow to the brain. If the degree of narrowing is severe, surgery may be needed to open the blood vessel.

A small spontaneous pneumothorax may resolve without treatment; a pneumothorax arising as a result of lung disease or injury requires immediate treatment. Treatment may include insertion of a chest tube or aspiration of the free air in the chest cavity.Feb 19, 2016
Biceps tenodesis surgery is performed when the biceps tendon is damaged, or the rotator cuff tendon or cartilage ring in the shoulder is torn. The biceps tendon is a strong rope‐like structure connecting the upper end of the biceps muscle to the bones in the shoulder. In biceps tenodesis surgery, the biceps tendon is separated from the shoulder and reattached to the humerus, or the upper arm bone.
General Neurological Exam Power Reflex Sensory Cranial erves

Recent researches shows that women with periodontal disease are more prone to deliver premature babies
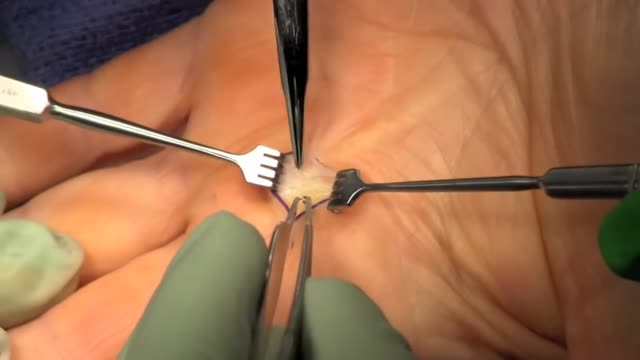
Trigger finger, also known as stenosing tenosynovitis (stuh-NO-sing ten-o-sin-o-VIE-tis), is a condition in which one of your fingers gets stuck in a bent position. Your finger may straighten with a snap — like a trigger being pulled and released. Trigger finger occurs when inflammation narrows the space within the sheath that surrounds the tendon in the affected finger. If trigger finger is severe, your finger may become locked in a bent position. People whose work or hobbies require repetitive gripping actions are at higher risk of developing trigger finger. The condition is also more common in women and in anyone with diabetes. Treatment of trigger finger varies depending on the severity.

Laparoscopic duodenal ulcer perforation repair 2

The video will describe the position of ET tube on a chest x-rays. Please see my website for disclaimer.

A video showing the accurate steps of Gloving, Gowning and Surgical Scrub

Flexor Digitorum Profundus (FDP) Finger Tendon Repair

An AV fistula is a connection, made by a vascular surgeon, of an artery to a vein.Vascular surgeons specialize in blood vessel surgery. The surgeon usually places an AV fistula in the forearm or upper arm. An AV fistula causes extra pressure and extra blood to flow into the vein, making it grow large and strong.
A peak flow meter is an inexpensive, portable, handheld device for those with asthma that is used to measure how well air moves out of your lungs. Measuring your peak flow using this meter is an important part of managing your asthma symptoms and preventing an asthma attack.
Thalassemia (thal-uh-SEE-me-uh) is an inherited blood disorder characterized by less hemoglobin and fewer red blood cells in your body than normal. Several types of thalassemia exist, including alpha-thalassemia, beta-thalassemia intermedia, Cooley's anemia and Mediterranean anemia. Hemoglobin is the substance in your red blood cells that allows them to carry oxygen. The low hemoglobin and fewer red blood cells of thalassemia may cause anemia, leaving you fatigued. If you have mild thalassemia, you may not need treatment. But, if you have a more severe form of thalassemia, you may need regular blood transfusions. You can also take steps on your own to cope with fatigue, such as choosing a healthy diet and exercising regularly.
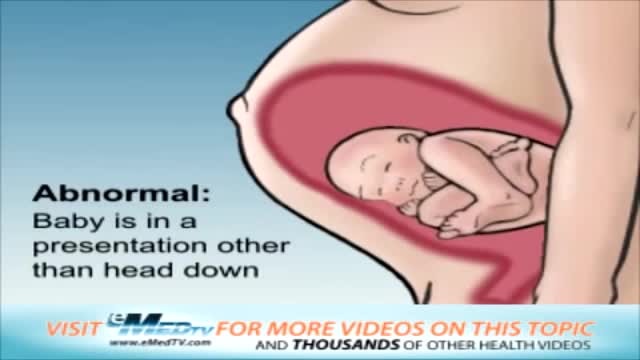
This video describes the various positions a baby may be in prior to delivery.
