- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
ACTUAL CATHETERIZATION A clinical view of insertion into the male urethra. A 14 french coude cath was used.
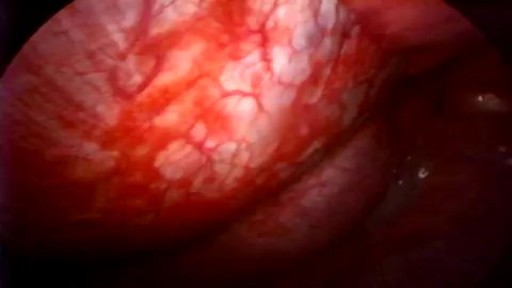
Video-assisted thoracoscopic talc pleurodesis is a highly effective technique to manage recurrent pneumothorax or pleural effusion.Surgical treatment using thoracoscopy may hasten postoperative recovery and reduce hospital stay.
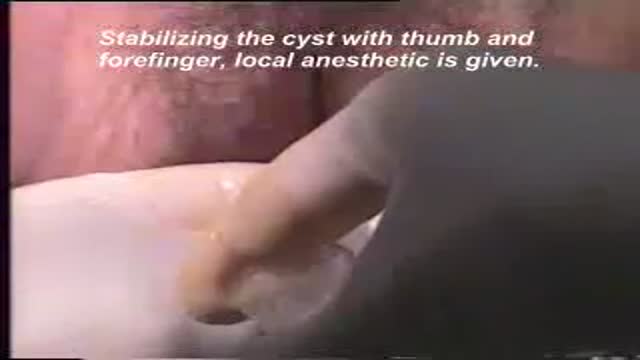
A video showing drainage of a bartholin cyst

Infected Tattoo Abscess

In this video, I am talking about the best histology resources available on the internet. All the links to the resources I talked are here -
1. Amit's lectures - https://www.youtube.com/channe....l/UCwdAyZnA6FEE0Iqsw
2. VIBS histology - https://www.youtube.com/c/VIBSHistology/featured
3. Dr. Eman Sadek Histology Queen - https://www.youtube.com/channe....l/UCHXGb5GphBKKN-xD3
4. BIOC 21 Histology lectures - https://www.youtube.com/playli....st?list=PLKnI3Jl97pW
5. https://medicalschoolpathology.com/
7. Udemy - https://clnk.in/qfEB
Buy this awsm book for Histology - https://amzn.to/3wSX1Oh

Dilatation and curretage technique.

Abortion real ghraphics

childbirth twin baby

Watch that video to know How to Insert Enema

http://drraewynteirney.com.au/video/
http://drraewynteirney.com.au/....about-dr-raewyn-teir
Dr Raewyn Teirney - fertility specialist and Gynaecologist in Sydney shows a video recording of a laparoscopy for a woman with infertility and pelvic pain.

Shave Your Pubic Hair

Examination of pulse, blood pressure and capillary refilling time

MRCPCH Clinical Revision - more videos at http://mrcpch.paediatrics.co.uk
Revise for your MRCPCH Clinical exam, with videos and high quality content created by the London Paediatrics Trainees Committee.
Examiner: Jonathan Round
Candidate: Amitav Parida
Filming: Mary Chesshyre, Huey Miin Lee, Chris Kelly
Thank you to the Evelina Children's Hospital for allowing us to film during their MRCPCH Revision Course (https://www.guysandstthomaseve....nts.co.uk/mrcpch-cli

Huge Sebaceous Cyst Removal Medical Video procedure

Watch that video to learn How to Insert Enema

Knee pain location can often tell you what type of knee pain you have. If you confirm that with common symptoms and what aggravates it… you can get a pretty good idea of ‘why my knee hurts’. So, here’s a quick look at the most common type of knee problems.
‘The 3 Essential Exercises EVERYONE Should Do’ … Watch this EXCLUSIVE video, only here: https://stefan-becker.mykajabi.com/3-essentials
QUESTIONS? I answer questions here now: I’ve started a Facebook Group to help people achieve their musculo-skeletal goals. Join here… https://www.facebook.com/groups/bodyfixexercises
AND I’m developing a Coaching Program! Over 12 weeks, I help people with posture related issues—like neck, shoulder, & upper back pain—discover their root problem and correct it using science-backed mobilising, stretching, & strengthening exercises… so they can feel straight, strong, flexible, & pain free again (and get back to doing what they love). Find out more, and join the wait list here… https://stefan-becker.mykajabi.com/waiting-list
0:00 Intro
0:11 Pain at the front of the knee (Pain in kneecap)
0:42 Pain below kneecap
1:40 Pain on inside of knee
3:05 Pain below knee on inside
3:29 Pain on outside of knee
3:28 Pain above knee
3:28 Pain behind knee
---------------------------------------
Mentioned in this video...
How To Fix Pain In The Front Of The Knee… (Runner's Knee) https://youtu.be/g0qmx_0enAA
Looking to stop your knee problems? Do this...
Knee Strengthening Exercises To Prevent Knee Pain
https://youtu.be/Pk-ae_lyx7M
How To Treat Patellar Tendinopathy (Jumper’s Knee) & Quadriceps Tendinopathy
https://youtu.be/MkPwsb-rQwU
---------------------------------------
If you’re asking yourself ‘what’s the cause of my knee pain?’ or ‘what kind of knee pain do I have?’ (so that you can look up solutions to your knee pain on YouTube) the position of your knee pain will tell you a lot.
THE MOST COMMON KNEE PAIN TYPES?
Knee pain during running (or actually kneecap pain while running) is usually just that… Runner’s Knee (PATELLOFEMORAL PAIN SYNDROME, or it’s old name: Chondromalacia Patella) If you get knee pain while cycling it will often be the same thing. Same with knee pain with stairs.
Knee pain while squatting could be Runner’s Knee, but if you get pain in the tendon below the kneecap, it’s more likely to be Patellar Tendonitis or Jumper’s Knee.
Meniscus Tears will give you pain on the inside of the knee that is a localised pain, can feel as if it gets stuck, or feel like it’s going to give way, and often it’s hard to fully straighten or fully bend your knee.
Knee pain on the outside of the knee is usually Iliotibial Band Syndrome
ALSO COVERED:
Infrapatellar Fat Pad Syndrome (Hoffa's Syndrome)
Osgood-Schlatter Disease
Medial Collateral Ligament Tear
Iliotibial Band Syndrome
Osteoarthritic Knee Pain
Pes Anserine Bursitis.
Quadriceps Tendinopathy
Popliteus Strain
Baker’s Cyst
ACL Or PCL Tear/Rupture
------------------------------------
#bodyfixexercises #kneepainrelief #kneepain
Anatomy of Love

How to remove the Intra Uterine Device (IUD)

Draining HUGE back abscess
Check out @barrettplasticsurgery on TikTok!
Like and subscribe for more! #shorts #medical #plasticsurgery
More information:
www.drdanielbarrett.com
