- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
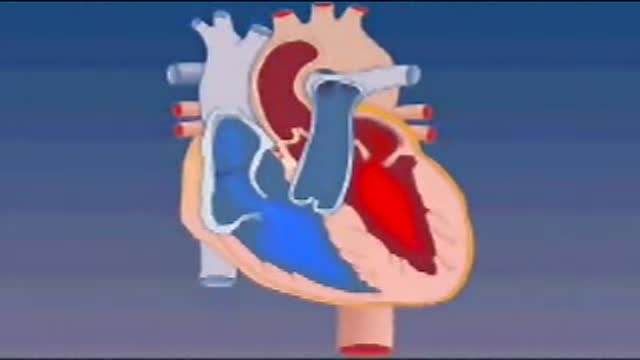
Blood enters the heart through two large veins, the inferior and superior vena cava, emptying oxygen-poor blood from the body into the right atrium. As the atrium contracts, blood flows from your right atrium into your right ventricle through the open tricuspid valve.
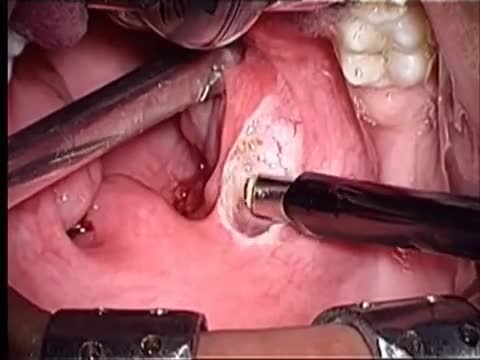
Tonsillectomy using coblation technique by wand Evac 70

There are several things to consider when trying to decide between gastric bypass surgery and gastric sleeve surgery. Unlike the laparoscopic adjustable gastric band (Lap Band), these two operations are both permanent, reduce hunger, and lead to the highest percentage of weight loss. To properly compare gastric sleeve surgery to gastric bypass surgery we will examine the following data : Expected weight loss. Speed of weight loss. Time of surgery. Gastric bypass benefits over sleeve. Gastric sleeve benefits over bypass. Risk of complications. Surgeon skill and preference.

A high definition HD video of Laparoscopic Cholecystectomy surgery
In some cases, the doctor will recommend that the couple seek assisted reproductive technologies (ART), such as IVF (in vitro fertilisation). ART do not cure or treat the cause of infertility but they can help couples achieve a pregnancy, even if the man's sperm count is very low.

Blepharitis is an inflammation of the eyelids in which they become red, irritated and itchy and dandruff-like scales form on the eyelashes. It is a common eye disorder caused by either bacteria or a skin condition, such as dandruff of the scalp or acne rosacea. It affects people of all ages. Although uncomfortable, blepharitis is not contagious and generally does not cause any permanent damage to eyesight.

Pulmonary edema is usually caused by a heart condition. Other causes include pneumonia, exposure to certain toxins and drugs, and being at high elevations. Depending on the cause, pulmonary edema symptoms may appear suddenly or develop over time. Mild to extreme breathing difficulty can occur. Cough, chest pain, and fatigue are other symptoms. Treatment generally includes supplemental oxygen and medications.

Orchitis (or-KIE-tis) is an inflammation of one or both testicles. It is usually caused by a bacterial infection or by the mumps virus. Bacterial orchitis can be caused by sexually transmitted infections (STIs), particularly gonorrhea or chlamydia. Bacterial orchitis often results from epididymitis, an inflammation of the coiled tube (epididymis) at the back of the testicle that stores and carries sperm. In that case, it's called epididymo-orchitis. Orchitis causes pain and can affect fertility. Medication can treat the causes of bacterial orchitis and can ease some signs and symptoms of viral orchitis. But it may take several weeks for scrotal tenderness to disappear.

When being overweight becomes more than just an inconvenience.

Mitral valve surgery is surgery to either repair or replace the mitral valve in your heart. Blood flows from the lungs and enters a pumping chamber of the heart called the left atrium. The blood then flows into the final pumping chamber of the heart called the left ventricle. The mitral valve is located between these two chambers. It makes sure that the blood keeps moving forward through the heart. You may need surgery on your mitral valve if: The mitral valve is hardened (calcified). This prevents blood from moving forward through the valve. The mitral valve is too loose. Blood tends to flows backward when this occurs. Minimally invasive mitral valve surgery is done through several small cuts. Another type of operation, open mitral valve surgery requires a larger cut.
This video show the steps in a total parotidectomy with VII nerve preservation. The patient had a malignant parotid tumor without VII nerve compromise.
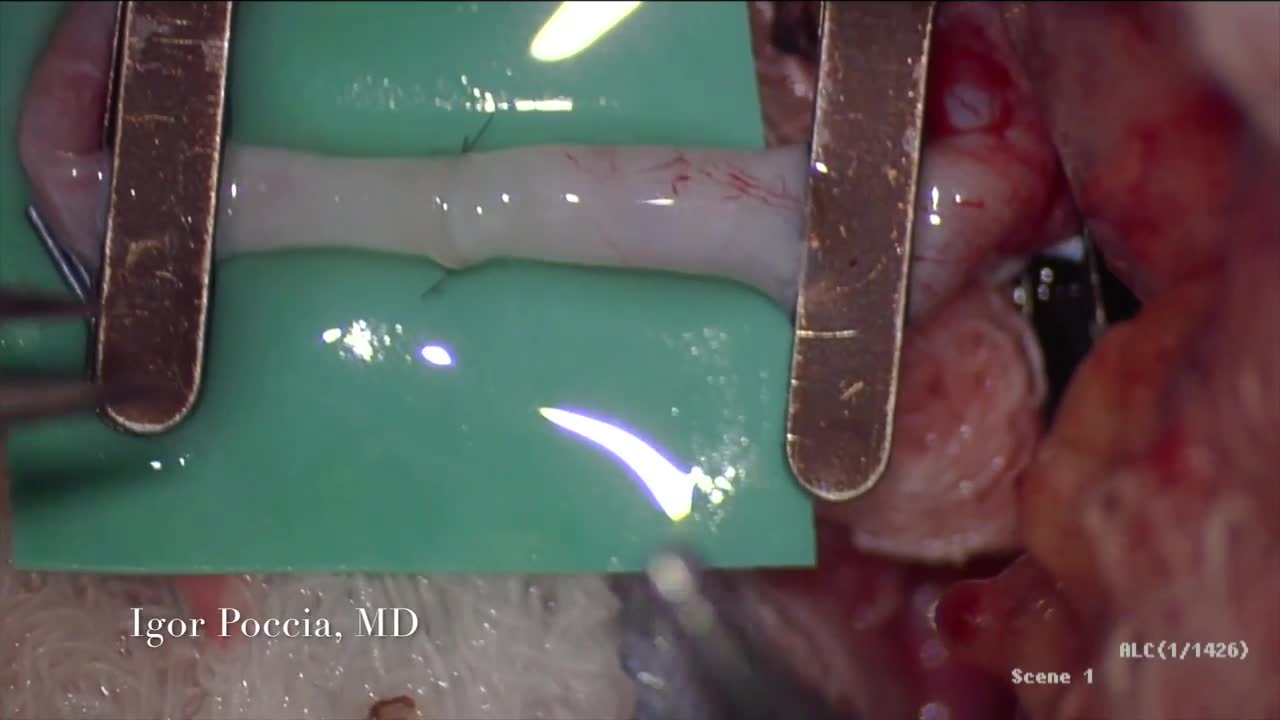
A circulatory anastomosis is a connection (an anastomosis) between two blood vessels, such as between arteries (arterio-arterial anastomosis), between veins (veno-venous anastomosis) or between an artery and a vein (arterio-venous anastomosis). An end artery (or terminal artery) is an artery that is the only supply of oxygenated blood to a portion of tissue. Examples of an end artery include the splenic artery that supplies the spleen and the renal artery that supplies the kidneys.
Hepatitis E is a virus that can infect the liver. Unlike other forms of hepatitis, the hepatitis E virus usually doesn't lead to long-term illness or serious liver damage. Most people get well within a few months.

Carpal Tunnel Syndrom 3D Animation
A narrowing of the major artery (the aorta) that carries blood to the body. This narrowing affects blood flow where the arteries branch out to carry blood along separate vessels to the upper and lower parts of the body. CoA can cause high blood pressure or heart damage.

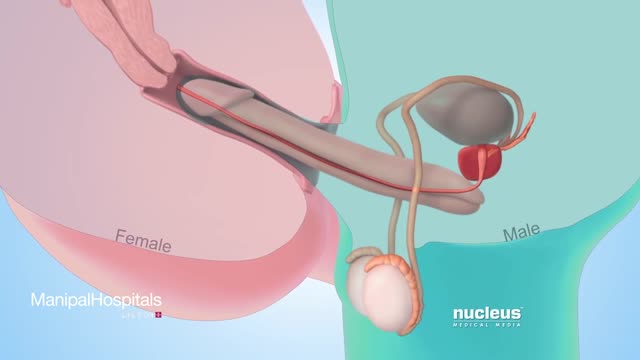
Most condoms are made of latex rubber, but they can also be made from lamb cecum or polyurethane. In addition to their contraceptive value, condom use has been found effective in preventing the spread of sexually transmitted diseases.

How to perform a parotidectomy gland resection? In this video we take you step by step through the protid gland resection surgical technique. This video is intended for ENT residents and Head and Neck Surgery Surgeons. It is part of the ORL-Information's Head and Neck surgery Masterclass in collaboration with the University Hospital of Nîmes. Surgeons Editors: Pr. Benjamin LALLEMANT, MD, PhD - Dr. Camille GALY, MD Head and and Neck Department, University Hospital of Nîmes, France Official video | www.orl-information.fr
Cette vidéo présentent la technique de la parotidectomie avec dissection du nerf facial. Elle illustre les différents temps de l'intervention notamment le temps de repérage du nerf facial.
--------------------------------------
@Prévention médecine | Comment préserver sa santé ?
✔Abonnez-vous à la chaîne ORL-Information : https://www.youtube.com/c/ORLINFORMATION
✔Retrouvez-nous sur internet: https://www.orl-information.fr

Contact us to find out more http://www.londonvisionclinic.com/contact-us/ Mr Carp explains the risks involved in losing sight as being extremely rare. Only 1 in 5 million may lose sight in one eye.
How to Perform Pregnancy Test at Home Video
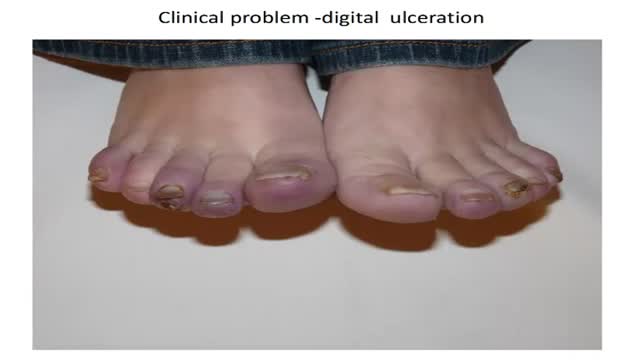
How to diagnose digital ulceration in out patient clinic.
