- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Endoscopic Removal of Coin from Esophagus
Overactive bladder syndrome is common. Symptoms include an urgent feeling to go to the toilet, going to the toilet frequently and sometimes leaking urine before you can get to the toilet (urge incontinence). Treatment with bladder training often cures the problem. Sometimes medication may be advised in addition to bladder training to relax the bladder.

emergency c-section for acute fetal distress, Misgav Ladach - modified Joel Cohen technique
The exact cause of schizophrenia isn't known, but genetics, environment, and imbalanced brain chemicals may play a role. Schizophrenia is characterized by abnormal social behavior. In severe cases, patients may see or hear things that aren't real. Treatment is usually lifelong and often involves a combination of medications and psychological and social therapy.
Electroconvulsive ECT Psychiatric Therapy Information

Colorectal cancer (also known as colon cancer, rectal cancer or bowel cancer) is the development of cancer in the colon or rectum (parts of the large intestine). It is due to the abnormal growth of cells that have the ability to invade or spread to other parts of the body. People with HNPCC tend to develop colon cancer before age 50. Familial adenomatous polyposis (FAP). FAP is a rare disorder that causes you to develop thousands of polyps in the lining of your colon and rectum. People with untreated FAP have a greatly increased risk of developing colon cancer before age 40.

A high definition HD video of Laparoscopic Cholecystectomy surgery

HPV causes genital warts and cervical and other anogenital cancers. The HPV vaccine is recommended for girls and women 9 to 26 years of age to reduce infections, but information on safety in pregnant women is limited.

Ascites, the collection of fluid within the peritoneal space is caused due to a variety of causes including cirrhosis, cardiac causes, sinusoidal obstruction syndrome, tubercular peritonitis and pancreatitis, amongst others. Most commonly, the cause of ascots may be cirrhosis , which in turn, is most frequently causes by alcohol use, hepatitis C and non-alcoholic steatohepatitis. At the heart of the ascitic fluid analysis is the serum albumin ascitic gradient, the differential diagnosis of which has been discussed in detail in this presentation. Both low SAAG and high SAAG ascites have been dealt with in some depth, with a brief overview of the management of these conditions

When being overweight becomes more than just an inconvenience.
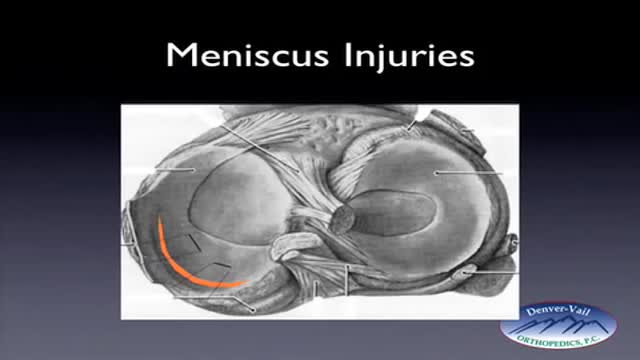
Rehabilitation time for a meniscus repair is about 3 months. A meniscectomy requires less time for healing — approximately 3 to 4 weeks. Meniscus tears are extremely common knee injuries. With proper diagnosis, treatment, and rehabilitation, patients often return to their pre-injury abilities.

Brain Concussion Accidents Examples

Carpal Tunnel Syndrome Information

Carpal Tunnel Syndrom 3D Animation

Tinnitus (TIN-ih-tus) is the perception of noise or ringing in the ears. A common problem, tinnitus affects about 1 in 5 people. Tinnitus isn't a condition itself — it's a symptom of an underlying condition, such as age-related hearing loss, ear injury or a circulatory system disorder


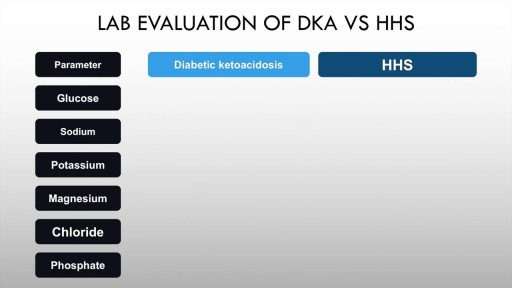
Diabetic ketoacidosis is an acute complication of uncontrolled hyperglycaemia characterised by high anion gap metabolic acidosis, dehydration and other metabolic abnormalities. Upto half of patients with Type 1 diabetes mellitus may have DKA. The incidence in T2DM is also rising. Precipitants include acute illness such as myocardial infarction, trauma and infection. Paitents of diabetic ketoacidosis may present with vomiting, pain abdomen and lethargy. Mental obtundation may also be present. Management of diabetic ketoacidosis revolves around administration of IV normal saline, insulin, replacement of potassium with frequent monitoring of sugars and electrolytes.
Watch that video to know How to Get Pregnant With Twins Naturally

Bell's palsy is a form of temporary facial paralysis resulting from damage or trauma to the facial nerves. The facial nerve-also called the 7th cranial nerve-travels through a narrow, bony canal (called the Fallopian canal) in the skull, beneath the ear, to the muscles on each side of the face. For most of its journey, the nerve is encased in this bony shell. Each facial nerve directs the muscles on one side of the face, including those that control eye blinking and closing, and facial expressions such as smiling and frowning. Additionally, the facial nerve carries nerve impulses to the lacrimal or tear glands, the saliva glands, and the muscles of a small bone in the middle of the ear called the stapes. The facial nerve also transmits taste sensations from the tongue. When Bell's palsy occurs, the function of the facial nerve is disrupted, causing an interruption in the messages the brain sends to the facial muscles. This interruption results in facial weakness or paralysis. Bell's palsy is named for Sir Charles Bell, a 19th century Scottish surgeon who described the facial nerve and its connection to the condition. The disorder, which is not related to stroke, is the most common cause of facial paralysis. Generally, Bell's palsy affects only one of the paired facial nerves and one side of the face, however, in rare cases, it can affect both sides.
